The Incretin-Myo Axis: Evaluating Tirzepatide’s Role in Lean Mass Retention during Rapid Adipose Atrophy Research
Discover how Tirzepatide leverages the Incretin-Myo Axis (the gut-muscle connection) to preserve lean muscle mass during rapid weight loss better than standard GLP-1s.
The Modern Weight Loss Dilemma: Dropping Fat vs. Losing Muscle
In the rapidly evolving world of health optimization and wellness biology, very few developments have changed the landscape quite like modern weight loss peptides. We have entered an era where shedding substantial amounts of body weight is no longer a roll of the genetic dice, but a predictable, scientifically manageable process. But as millions of people successfully shed pounds of unwanted body fat, a silent and incredibly important issue has stepped into the spotlight: the loss of lean muscle mass.
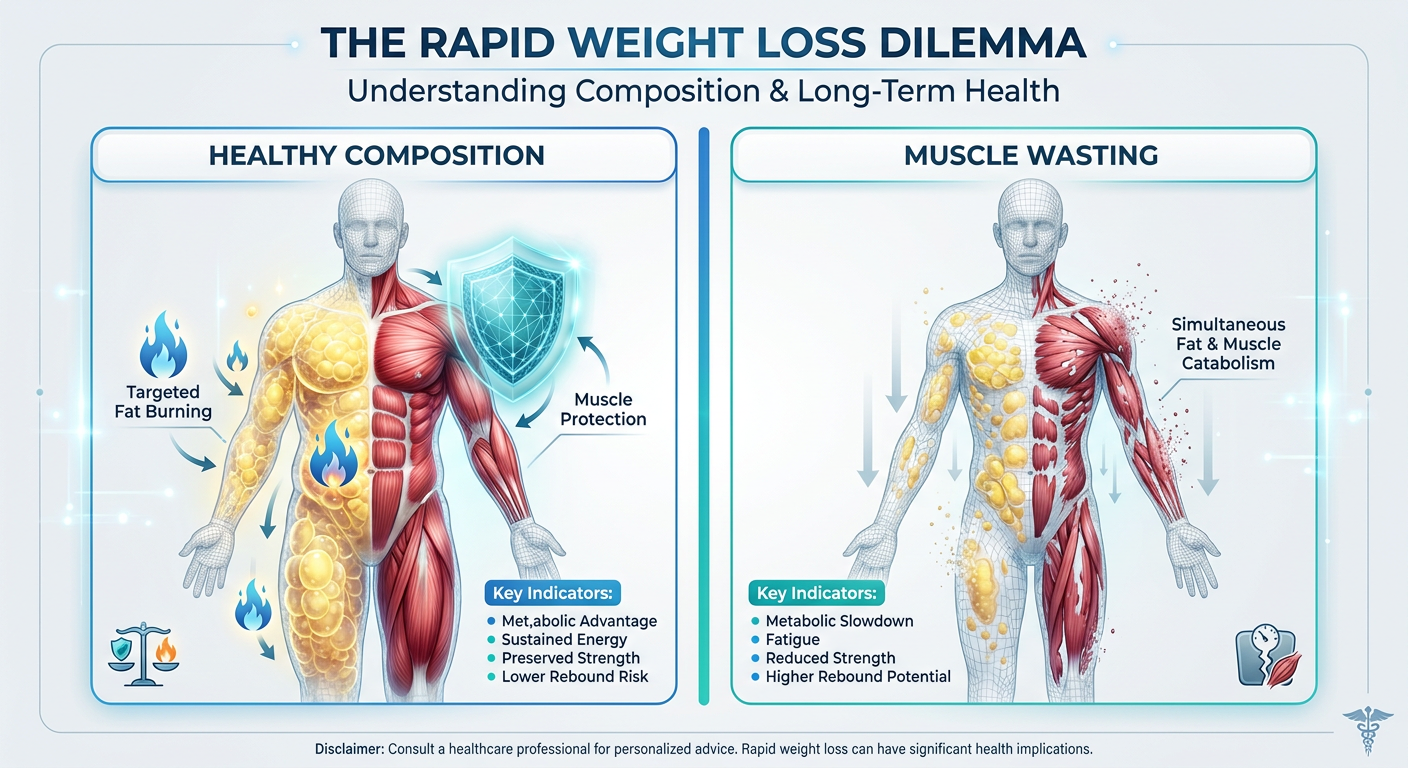
When the body rapidly burns off fat—a process clinical researchers refer to as "rapid adipose atrophy"—it is rarely a perfectly isolated event. Without the right physiological signals, a body in a steep caloric deficit will unfortunately burn through a mix of both fat and precious muscle tissue. This brings us to the most vital question in modern metabolic science: How do we tell the body to torch body fat without breaking down the muscle we need for health, metabolism, and longevity?
Enter the Incretin-Myo Axis. Simplified, this is the biochemical communication highway between your gut hormones (incretins) and your muscle tissue (myo). Understanding this connection is the key to preserving your strength, your metabolic rate, and your physical resilience while losing weight. And at the exact center of this breakthrough science sits Tirzepatide—a revolutionary dual-receptor agonist that is rewriting the rules on how we approach healthy body composition.
In this comprehensive guide, we are going to break down the science of the Incretin-Myo Axis in simple, actionable terms. We’ll explore why Tirzepatide is showing uniquely powerful muscle-sparing properties, how it compares to first-generation options, and how you can optimize your own health journey to ensure the weight you lose is strictly the weight you want gone.
What is Rapid Adipose Atrophy? (And Why It’s Not Just About Looking Good)
Let’s start by demystifying some clinical language. "Rapid Adipose Atrophy" might sound like a severe medical condition, but in research terms, it simply translates to fast, purposeful fat loss. "Adipose" refers to your body fat tissue, and "atrophy" means the shrinking or reduction of that tissue. So, when subjects in weight loss studies drop 15% to 20% of their body weight in just a few months, they are experiencing rapid adipose atrophy.
On paper, this sounds fantastic. If you have been carrying excess weight for years, the concept of rapid adipose atrophy is exactly what you are searching for. However, human biology evolved specifically to prevent this from happening. For millions of years, our bodies considered rapid fat loss to be a signal of starvation and extreme danger. To survive periods of famine, the human body developed a brutal defense mechanism: if food is scarce, the body slows down the metabolism by sacrificing calorie-hungry muscle tissue.
The Steep Price of Poorly Managed Weight Loss
Muscle is highly metabolically active. Even while you sit on the couch watching television, your muscle fibers are constantly burning calories simply to exist. Fat, conversely, is relatively dormant; it acts essentially like biological savings accounts, storing energy for later use. When you dramatically cut your food intake (which naturally happens when using appetite-suppressing peptides), your body assesses the situation and often decides that maintaining costly muscle tissue is a luxury it can no longer afford.
This biological accounting error leads to a phenomenon known as sarcopenic obesity, or what pop culture unfortunately refers to as being "skinny fat." You might weigh less on the scale, but your body composition—your ratio of muscle to fat—remains poor. Worse yet, because you have less muscle, your resting metabolic rate severely drops. If and when you stop your weight loss protocol, the lack of metabolic furnace (muscle) means rapid, aggressive weight regain.
Here is why maintaining lean mass is non-negotiable for long-term health:
- Metabolic Rate Protection: Muscle dictates how many calories you burn at rest. Losing muscle means you have to eat less forever just to maintain your new lower weight.
- Bone Density Support: Muscles pull on bones, stimulating them to stay dense and strong. Muscle loss is almost always correlated with a decrease in bone mineral density.
- Insulin Sensitivity: Your skeletal muscles act as giant sponges for blood sugar. The less muscle you have, the harder your body has to work to manage blood glucose levels, leading to insulin resistance.
- Functional Independence: Vitality, energy levels, posture, and strength depend on healthy muscle tissue. You want to age like a finely tuned athlete, not a frail shadow of your former self.
The Baseline: Pure GLP-1 Agonists and Their Limitations
Before we can truly appreciate the innovation of Tirzepatide, we have to look at the generation of peptides that paved the way. You have almost certainly heard of pure GLP-1 receptor agonists, with the most famous being Semaglutide.
GLP-1 (Glucagon-Like Peptide-1) is a naturally occurring incretin hormone secreted by your intestines right after you eat a meal. It travels to your brain to signal that you are full, it slows down the rate at which your stomach empties (gastric emptying) so you feel full longer, and it prompts your pancreas to release a highly calibrated amount of insulin to handle the incoming food.
As a weight loss tool, GLP-1 agonists are undeniably effective. They quiet "food noise," completely eliminate cravings, and allow individuals to effortlessly maintain the steep caloric deficit required for massive weight loss. But they work almost too well. Because they are so highly effective at crushing appetite, users often accidentally drop their daily protein intake to dangerously low levels.
And here is the critical flaw of pure GLP-1 therapy: GLP-1 receptors primarily exist in the brain, the gut, and the pancreas. They do not have a strong, direct line of communication with skeletal muscle tissue. Semaglutide essentially tells the brain to stop eating, but it provides no inherent biochemical signal telling the body to preserve lean muscle tissue while the weight comes off. Muscle preservation on a pure GLP-1 is completely dependent on the user fighting an uphill battle: strictly forcing themselves to eat high amounts of protein and lifting heavy weights despite having zero appetite.
Enter Tirzepatide: The Power of GIP and Dual-Action Synergy
This brings us to the absolute cutting edge of metabolic peptide science: Tirzepatide. Unlike first-generation peptides, Tirzepatide doesn’t just mimic one hormone; it mimics two. It is a "dual-agonist" that targets both the GLP-1 receptor and the GIP receptor.
GIP stands for Glucose-Dependent Insulinotropic Polypeptide (historically referred to as Gastric Inhibitory Polypeptide). For decades, researchers largely ignored GIP, believing it was just a weaker, less important sibling to GLP-1. But modern peptide mapping revealed a shocking truth: GIP is actually a profoundly powerful metabolic conductor, especially when it comes to regulating how the body stores and utilizes fat and sugar.
By engineering a single peptide that activates both receptors, researchers achieved what is known in biology as "synergy." The whole became massively greater than the sum of its parts. Tirzepatide utilizes GLP-1 to control appetite and slow digestion, but it unleashes GIP to communicate directly with fat cells (adipocytes) and, crucially, skeletal muscle tissue. This dual signaling is what creates the Incretin-Myo Axis.
The Incretin-Myo Axis: The Secret to Protecting Muscle
So, how exactly does the addition of GIP change the game for human body composition? The magic lies in where GIP receptors are located in the human body. While GLP-1 isolates its action primarily to the brain and gut, GIP receptors are incredibly abundant on the surface of white adipose tissue (fat cells) and are heavily involved in the vascular and nutrient-partitioning pathways that feed our skeletal muscle.
When Tirzepatide activates this Incretin-Myo pathway, several complex scientific processes occur, which we can translate perfectly into real-world benefits for your body:
1. Nutrient Partitioning: Shuttling Fuel to Muscle
Think of your body as a large nightclub, and the nutrients you eat (carbohydrates and fats) are the guests trying to get in. Insulin is the bouncer who decides where those guests go. In a normal, mildly insulin-resistant person, the bouncer forcefully shoves the majority of incoming calories into the VIP room (fat cells) and barely lets anything into the main dance floor (muscle cells). This makes you gain fat easily while making it incredibly hard to build or maintain muscle.
The GIP component of Tirzepatide fundamentally retrains the bouncer. GIP dramatically increases insulin sensitivity precisely at the cellular level. By doing so, it improves "nutrient partitioning." It tells your body to divert incoming glucose and amino acids away from fat storage and forces them into skeletal muscle tissue. Because your muscles are being actively fed and hydrated at a cellular level, your body is biologically discouraged from breaking them down, even if your total daily calories are extremely low.
2. Enhanced Fat Oxidation (Sparing Protein)
When the body needs energy, it has three fuel tanks to choose from: carbohydrates (glycogen), fats (lipids), and proteins (muscle). Rapid weight loss requires the body to dip heavily into its reserves. Pure caloric restriction often forces the body to burn a dangerous mix of fat and muscle-derived protein.
Tirzepatide changes your fuel preference. Through the activation of GIP receptors on white adipose tissue, the peptide encourages the healthy release and rapid oxidation (burning) of stored fat. It essentially turns fat into the path of least resistance for energy. Because fat becomes so easily accessible as a fuel source, the body no longer feels the "starvation panic" that forces it to cannibalize muscle proteins. The muscle is spared because the fat is doing its job.
3. Reducing Systemic Inflammation
A hidden enemy of muscle growth and retention is chronic, low-grade inflammation. Excess body fat is essentially a toxic organ, constantly pumping inflammatory cytokines into your bloodstream. This inflammation actively blocks muscle protein synthesis (the process of building and repairing muscle). Recent research indicates that GIP signaling has powerful anti-inflammatory effects in the body. By cooling this systemic inflammation, Tirzepatide creates a far more hospitable internal environment (a healthier host, in clinical terms) for muscle maintenance.
The Data: Tirzepatide vs. Semaglutide in Body Composition
Science is fascinating, but tangible data is what actually matters to your health journey. When we look at the clinical trials for these peptides, we see stark differences in the quality of the weight being lost.
In standard bariatric surgery or extreme starvation dieting, it is not uncommon for a person to lose 100 pounds, but completely tragically, 30 to 40 pounds of that was pure lean muscle mass. They become a smaller, but mechanically weaker and less metabolically stable version of themselves.
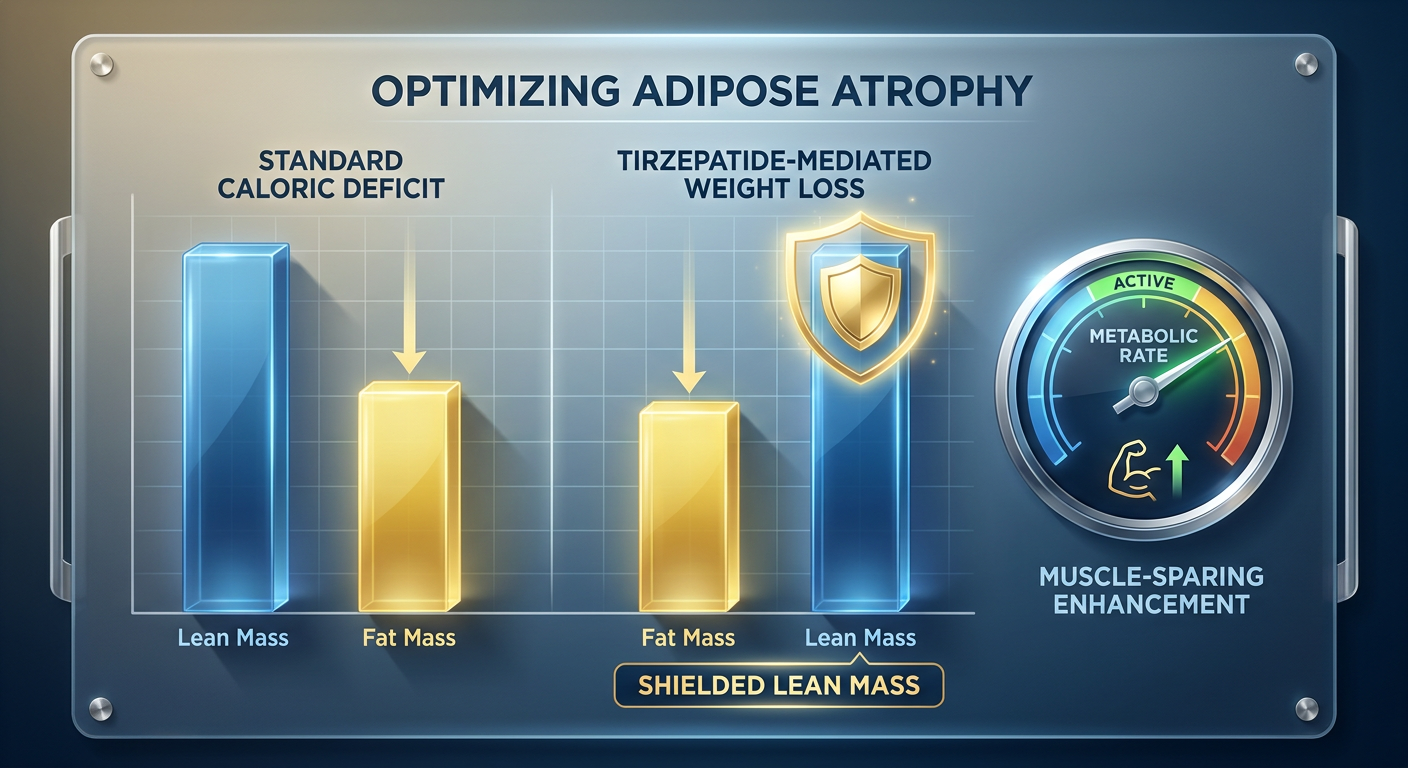
During the STEP clinical trials for Semaglutide, researchers observed phenomenal total body weight loss, but DEXA scans (advanced body composition imaging) occasionally showed lean mass losses hovering around 35% to 40% of the total weight lost in subjects who didn't explicitly resistance train. Again, to be fair to Semaglutide, this is standard for rapid weight loss without protein enforcement, but it is not optimal.
Then came the SURMOUNT clinical trials for Tirzepatide. The results astounded researchers in two ways. First, the absolute volume of weight lost was unprecedented—rivaling surgical interventions. But more importantly, body composition MRIs revealed that the ratio of fat mass lost compared to lean mass lost was remarkably more favorable. Only about 25% of the total weight lost was lean mass. Wait, you might ask, isn't 25% muscle loss still bad? In clinical research involving massive double-digit percentages of body weight loss without enforced exercise, a 3-to-1 ratio of fat loss to lean mass loss is considered excellent, and it represents a massive upgrade in tissue preservation compared to older protocols.
Comparison Table: Weight Loss Peptides & Body Composition
| Method / Compound | Primary Mechanism | Average % of Total Weight Loss | Lean Mass Preservation Rating |
|---|---|---|---|
| Standard Dieting | Caloric restriction through willpower | 5 - 10% (High rebound rate) | Moderate (Highly dependent on protein intake) |
| Bariatric Surgery | Physical stomach reduction | 25 - 35% | Very Poor (Severe malabsorption of protein) |
| Semaglutide | GLP-1 Receptor Agonist | 15 - 17% | Moderate (Appetite suppression lowers protein intake) |
| Tirzepatide | GLP-1 + GIP Receptor Agonist | 20 - 24% | High (Incretin-Myo Axis improves nutrient partitioning) |
Next-Generation Upgrades: The Horizon of Obesity Peptides
The success of the dual-agonist approach utilized by Tirzepatide fundamentally proved that stacking receptor signals creates better metabolic outcomes. This realization has set off a golden age of peptide development, bringing forth new compounds that aim to preserve muscle even better while pushing fat mobilization to the absolute limit.
The Co-Agonist Blends: Cagrilintide + Semaglutide
While Tirzepatide uses one molecule to hit two receptors, another powerful approach involves blending two separate powerful peptides to create a synergistic metabolic environment. One of the most exciting developments in this space is the Cagrilintide + Semaglutide Blend. Cagrilintide is a long-acting amylin analog. Amylin is a hormone co-secreted with insulin that heavily regulates satiety and glucagon release. When you pair the intense appetite control of Semaglutide with the deep metabolic recalibration of Cagrilintide, researchers are observing weight loss metrics that meet or even exceed Tirzepatide, with early indications suggesting excellent preservation of mechanical force—meaning subjects keep their strength.
The Triple-Agonists: Introducing Retatrutide
If two targets are better than one, what about three? This is where Retatrutide steps onto the scene. Retatrutide is a "Tri-Agonist" targeting the GLP-1, GIP, and Glucagon receptors. The addition of the Glucagon receptor is a masterstroke in metabolic engineering. Glucagon directly heavily stimulates energy expenditure. It forces the liver to burn stored fat for energy and actively increases basal metabolic heat (thermogenesis). The theory is that by vastly increasing the amount of energy the body is forced to burn while simultaneously using GIP to protect the muscle, Retatrutide may represent the absolute pinnacle of rapid, metabolically safe adipose atrophy.
Stacking for Success: How to Actively Protect Your Lean Mass
Even with the advanced Incretin-Myo Axis communication provided by Tirzepatide, passive health optimization leaves results on the table. The most successful protocols recognize that weight-loss peptides should act as the foundation, while other specific amino acid sequences and lifestyle protocols act as the specialized tools for muscle retention.
Researchers and wellness optimizers routinely look to specific, targeted pathways to promote muscle protein synthesis while in a caloric deficit.
1. Stimulating Growth Hormone (The Ultimate Muscle Protector)
Human Growth Hormone (HGH) is one of the body’s most powerful anti-catabolic (muscle-sparing) substances. Elevated HGH practically forbids the body from cannibalizing muscle tissue while simultaneously forcing fat cells to empty their lipid payloads. However, direct synthetic HGH can disrupt endogenous production. The far smarter route is using Growth Hormone Secretagogues (GHS)—peptides that tell your own pituitary gland to naturally pulse out massive amounts of your own growth hormone.
Peptides like Ipamorelin and Tesamorelin are considered elite tier for this exact purpose. Using them alongside Tirzepatide creates a highly optimized internal environment: Tirzepatide controls the appetite and improves insulin sensitivity, while the GH secretagogue actively repairs, defends, and sometimes even builds lean muscle tissue during the weight-loss phase.
2. The Mitochondrial Bio-Energy Fix
Weight loss can sometimes cause profound fatigue, and when you are tired, you don't engage your muscles. Muscle tissue is densely packed with mitochondria—the biological power plants of your cells. As we age, or as we endure metabolic stress, these power plants become highly dysfunctional. Peptides that specifically target mitochondrial health operate deeply inside the muscle cell to restore energy and functional strength.
Mitochondrial-derived peptides like MOTS-c, as well as the revolutionary small molecule 5-Amino-1MQ, act as cellular exercise mimetics. They activate an enzyme called AMPK, tricking the body into acting as if it is performing vigorous cardiovascular exercise. This process drastically increases cellular energy, burns intra-muscular fat (the dangerous fat hiding inside the muscle tissue itself), and radically improves endurance. Retaining muscle is much easier when your muscle cells are producing peak amounts of ATP (energy).
3. Rapid Tissue Repair and Cellular Healing
To retain muscle, you have to use it. Resistance training is universally required. But heavy resistance training causes micro-tears in the muscle and stress on the tendons. Under the extreme low-calorie conditions triggered by GLP-1 / GIP agonists, your body's ability to heal connective tissue suffers significantly. This is why incorporating a powerful regenerative peptide like BPC-157 into a protocol is deeply popular. BPC-157 massively accelerates angiogenesis (the creation of new blood vessels), routing vital healing nutrients directly to damaged muscle and tendons, ensuring you can maintain the heavy lifting needed to hold onto your mass.
Stacking Synopsis Matrix: Peptide Synergy
| Goal Focus | Primary Agent | Synergistic Partner | Biological Result |
|---|---|---|---|
| Maximum Fat Loss + Muscle Preservation | Tirzepatide | Tesamorelin | Incretin-driven fat reduction combined with GH-mediated lipolysis and extreme muscle defense. |
| Appetite Crushing + Cellular Energy | Semaglutide | 5-Amino-1MQ | Blocks hunger centrally while ramping up peripheral metabolic rate and intra-muscular energy production without stimulants. |
| Recovery + Extreme Tissue Protection | Tirzepatide | BPC-157 + MK-677 (Ibutamoren) | GIP prevents muscle wasting while BPC repairs joint/tissue damage and MK-677 provides sustained IGF-1 release for whole-body anabolism. |
The "Meat and Potatoes": Lifestyle Rules for the Incretin-Myo Axis
While peptides are incredibly powerful metabolic conductors, they are ultimately signaling systems. You still have to provide the raw materials. If you use Tirzepatide but starve yourself of protein and never lift a single weight, you will still lose a tragic amount of muscle. You cannot cheat the fundamental laws of thermodynamics and biological adaptation.
To optimize the Incretin-Myo Axis and ensure a flawless body recomposition, you must adhere to these three uncompromising rules:
- Protein is Your Non-Negotiable Armor: When your appetite vanishes due to GLP-1/GIP signaling, the single most important macronutrient to prioritize is protein. Aim for roughly 0.8 to 1.0 grams of high-quality protein per pound of your ideal body weight. If you can only eat a few bites before feeling stuffed, those bites must be lean meats, eggs, or clean protein supplements. Carbohydrates and fats are merely fuel; protein is the structural building block of your body.
- Lift Heavy Things (Mechanical Tension): Muscle is an adaptation to stress. If you do not provide a stimulus (lifting weights) that forces the body to keep the muscle, no peptide on earth will fully save it. You do not need to become a bodybuilder. Lifting weights merely 3 to 4 days a week focusing on heavy, compound movements (squats, deadlifts, presses, rows) sends a massive biological signal: "Do not burn this tissue; I am actively using it to survive."
- Prioritize Hydration and Electrolytes: Rapid fat loss dumps massive amounts of water and intracellular minerals. Decreased food intake also limits your incidental sodium and potassium intake. Cramping, weakness, and loss of muscular force (strength) frequently happen not because you lost muscle, but because your muscles are dehydrated and lack the electrolytes necessary to contract properly. Drink water vigorously, and salt your food.
The Absolute Necessity of High-Tier Purity
A very serious conversation that researchers and health enthusiasts must have is the topic of peptide purity. When you are studying intricate biological systems like the Incretin-Myo Axis, introducing degraded, impure, or poorly synthesized compounds into your protocol isn't just a waste of money—it is highly counterproductive. It can trigger harsh immune responses, severe injection site reactions, and entirely negate the delicate metabolic partitioning you are trying to activate.
The peptide industry has unfortunately become flooded with low-tier suppliers cutting corners. You must insist on rigorous quality control. A premium supplier like Alpha Carbon Labs doesn't just make claims; they prove it.
Every single batch of research biomaterials must be backed by verifiable, third-party COA (Certificate of Analysis) documents. These reports confirm the exact nanogram dosage of the vial and verify that the product is completely clean of dangerous heavy metals, endotoxins, and leftover manufacturing impurities. Finally, understanding the methodology behind advanced peptide synthesis reveals why true, clinical-grade chains cost what they do. You are fundamentally paying for molecular precision, which is the exact same precision deciding whether you burn body fat or your own heart and skeletal muscle.
Advanced FAQ: Mastering Tirzepatide and Muscle Health
1. Is it normal to feel weaker when I start using Tirzepatide?
In the first few weeks, a mild reduction in energy and gym performance is normal, but it is rarely due to actual muscle loss. Instead, because your carbohydrates are dropping drastically, your intramuscular glycogen (stored sugar in the muscle) depletes. Glycogen holds water. When your muscles empty out the sugar and water, they feel "flat," and you lose mechanical leverage, which can make you feel weaker. This is an energy-substrate issue, not a literal muscle-wasting issue. As your body adapts to burning fat and utilizing GIP’s insulin-sensitizing effects, your strength should stabilize.
2. Can I actually build new muscle while on Tirzepatide?
This is what the fitness industry calls "body recomposition," and yes, it is entirely possible, though very difficult. It typically only happens under three conditions: you are relatively new to weightlifting (a state known as "newbie gains"), you are returning from a long break (muscle memory), or you have a significantly high body fat percentage to start with. In these scenarios, the body can successfully harness the massive energy stored in your fat cells and use it to fuel the construction of new muscle tissue, provided your daily protein intake is exceptionally high. The GIP signaling from Tirzepatide makes this unique metabolic partition vastly more achievable compared to pure starvation dieting.
3. Why shouldn't I just use Semaglutide if it's cheaper?
Semaglutide is a phenomenal, life-changing peptide for millions of people. It forcefully controls appetite and regulates blood sugar. If sheer cost is paramount and you are perfectly disciplined with your diet and weightlifting routine, Semaglutide is a highly viable path. However, you are sacrificing the Incretin-Myo Axis. You are losing the direct GIP communication that acts as an invisible safety net for your lean mass. You are also missing out on the superior tolerability; because Tirzepatide uses dual pathways, many users report significantly lower rates of nausea and gastrointestinal distress compared to high-dose pure GLP-1s.
4. Does targeting mitochondria with peptides like SS-31 help with muscle tone?
Absolutely. Peptides like SS-31 are designed to restore the inner mitochondrial membrane (specifically targeting a lipid called cardiolipin). When you are rapidly dropping weight, oxidative stress increases rapidly. By restoring mitochondrial efficiency, SS-31 ensures that your existing muscle cells can optimally process oxygen and nutrients. This translates into less muscular fatigue during your workouts, allowing you to train harder, which inherently protects your lean mass from atrophy.
5. When is the best time to run a peptide cycle for muscle preservation?
Peptide use is deeply personal and dependent on your specific research goals. However, most experts agree that protecting the muscle is a full-time job. It is highly beneficial to overlap your protocols. Using Tirzepatide consistently to manage weight loss, while doing a targeted 8-to-12-week intensive cycle of an HGH secretagogue (like Ipamorelin) during the steepest phase of your caloric deficit, often yields the most striking body composition changes. Always remember to cycle off hormonal secretagogues safely to maintain natural pituitary function.
Conclusion
The evolution from blunt-force starvation dieting to targeted metabolic signaling represents a beautiful leap forward in human biological optimization. Rapid Adipose Atrophy—losing massive amounts of fat—no longer has to be a double-edged sword that strips away your hard-earned muscle, bone density, and metabolic speed.
By understanding the Incretin-Myo Axis, we realize that the body needs direct instructions to partition nutrients effectively. Tirzepatide’s brilliant combination of GLP-1 for appetite control and GIP for muscular insulin sensitivity and fat oxidation has set a new gold standard in weight management. When you source high-purity compounds, commit firmly to adequate protein intake, engage in dedicated resistance training, and intelligently stack supportive mitochondrial and growth hormone peptides, you truly gain ultimate control over your physical architecture. You are not just losing weight; you are unveiling the strongest, most vital version of yourself.
References
- 1. Jastreboff, A. M., et al. (2022). Tirzepatide Once Weekly for the Treatment of Obesity. The New England Journal of Medicine, 387(3), 205–216.
- 2. Wilding, J. P. H., et al. (2021). Once-Weekly Semaglutide in Adults with Overweight or Obesity. The New England Journal of Medicine, 384(11), 989–1002.
- 3. Rosenstock, J., et al. (2021). Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): a double-blind, randomised, phase 3 trial. The Lancet, 398(10295), 143-155.
- 4. Heise, T., et al. (2022). Tirzepatide reduces appetite, energy intake, and fat mass in people with type 2 diabetes. The American Journal of Clinical Nutrition, 115(5), 1339–1349.
- 5. Finan, B., et al. (2013). Unimolecular dual incretins maximize metabolic benefits in rodents, monkeys, and humans. Science Translational Medicine, 5(209), 209ra151.
- 6. Samms, R. J., et al. (2020). GIPR agonism mediates weight loss and metabolic benefits of a dual GIP/GLP-1 agonist. Nature Metabolism, 2(10), 1083–1093.
- 7. Campbell, J. E. (2021). Targeting the GIP receptor for obesity: To agonize or antagonize? Cell Metabolism, 33(1), 29-31.
- 8. Cusi, K., et al. (2021). Effect of tirzepatide on ectopic fat and insulin sensitivity in people with type 2 diabetes (SURPASS-3 MRI): a phase 3, randomised, open-label, parallel-group trial. The Lancet Diabetes & Endocrinology, 9(6), 332-344.
- 9. Willard, F. S., et al. (2020). Tirzepatide is an imbalanced and biased dual GIP and GLP-1 receptor agonist. JCI Insight, 5(17), e140532.
- 10. Mathiesen, D. S., et al. (2019). The Effects of GIP on Satiety and Food Intake. Nutrients, 11(11), 2658.
All research information is for educational purposes only. The statements made within this website have not been evaluated by the US Food and Drug Administration. The statements and the products of this company are not intended to diagnose, treat, cure or prevent any disease.