Scaling Receptor Affinity: A Technical Guide to Comparative Molar Dosing in Next-Generation Incretin Research
Discover how to navigate the transition between advanced weight loss peptides. This comprehensive guide breaks down receptor affinities and comparative dosing when upgrading from Semaglutide to next-generation powerhouses like Tirzepatide and Retatrutide.
Scaling Receptor Affinity: A Technical Guide to Comparative Molar Dosing in Next-Generation Incretin Research
The title of this article sounds like it belongs in a dense biology textbook, doesn't it? "Scaling receptor affinity," "comparative molar dosing," and "next-generation incretins" are terms that can make even a seasoned wellness enthusiast's eyes glaze over. But here is the reality: if you are interested in the cutting edge of weight loss, metabolic health, and anti-aging, understanding these concepts is the key to unlocking the body of your dreams.
In plain English, we are talking about the evolution of the world's most famous weight loss peptides. We refer to the transition from first-generation tools like Semaglutide (a single-target peptide), to dual-action powerhouses like Tirzepatide, and finally to the astonishing new frontier of triple-action peptides like Retatrutide.
When transitioning from an older peptide to a newer, stronger one, you cannot simply swap your dosage milligram for milligram. Why? Because these new formulas bind to your body's cells differently—they have distinct "cellular lock-and-key" mechanisms, or as scientists call it, different receptor affinities. Understanding how to transition smoothly, safely, and effectively between these compounds will ensure you keep shedding fat, protecting your muscle tone, and feeling energized throughout your health journey.
Whether you are a deep-dive biohacker studying your own metabolic data, or simply a health-conscious adult looking to finally beat leptin resistance and shed stubborn pounds, this guide will translate complex incretin science into highly actionable, real-world strategies.
The Evolution of Weight Loss: From GLP-1 to the Tri-Agonists
To understand how to dose these compounds, we first have to understand what they are actually doing inside your body. Over the last decade, a specific class of peptides called "incretins" has completely revolutionized obesity research, anti-aging, and general wellness.
Incretins are natural metabolic hormones your gut releases when you eat. They tell your brain you are full, prompt your pancreas to release insulin to handle sugar, and slow down your digestion so you feel satisfied longer. In the peptide world, researchers have synthesized powerful, long-lasting versions of these incretins. They act as "agonists," meaning they successfully trigger these beneficial responses in your body, but with far greater strength and for a much longer duration than your natural hormones.
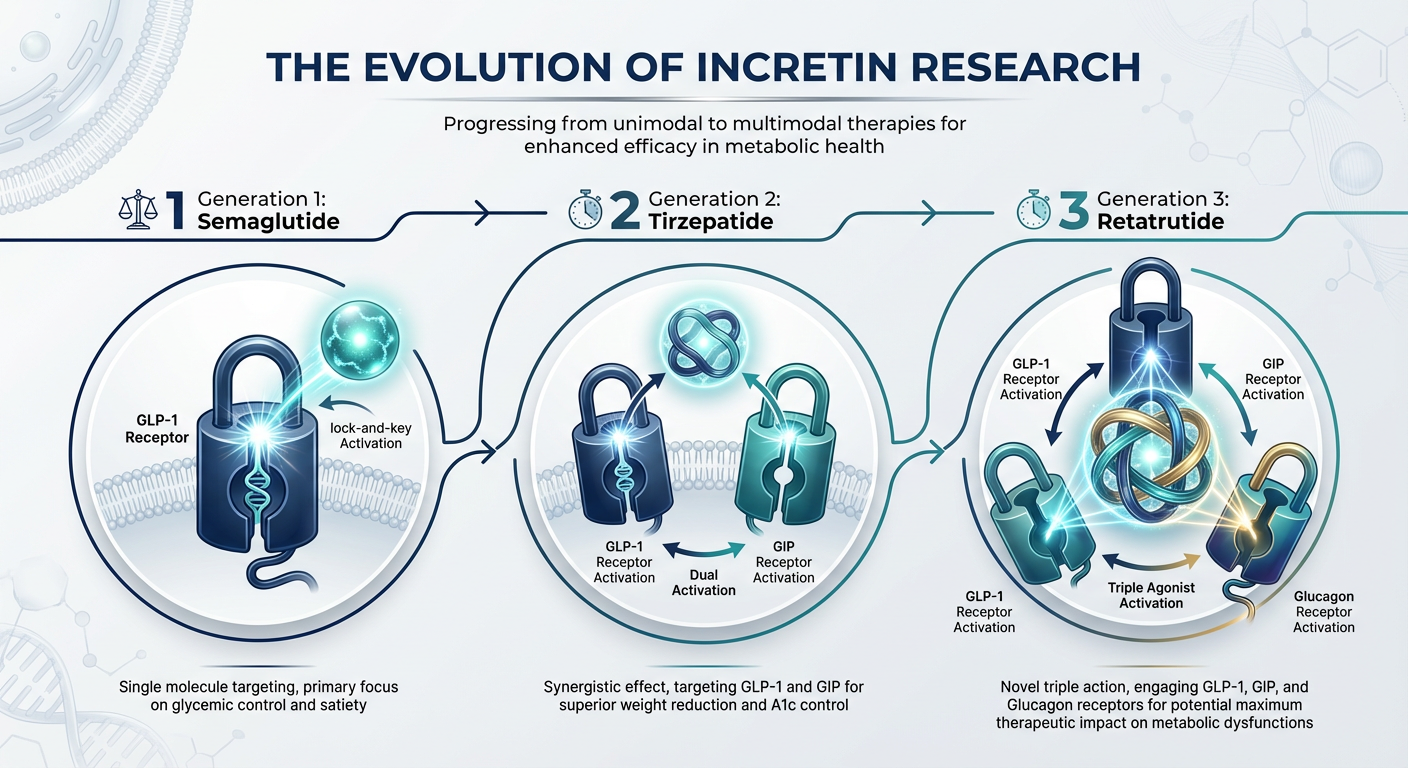
The evolution of these peptides happened in three distinct waves:
- Generation 1: Single-Receptor Agonists (GLP-1). This is where it all started. Peptides like Semaglutide target exactly one cellular pathway: the Glucagon-Like Peptide-1 (GLP-1) receptor. Their superpower is shutting down your appetite and eliminating "food noise"—those obsessive thoughts about your next meal.
- Generation 2: Dual-Receptor Agonists (GLP-1 + GIP). Researchers quickly asked, "What if we target two pathways at once?" Tirzepatide was born. It activates both GLP-1 and Glucose-Dependent Insulinotropic Polypeptide (GIP). This duo not only kills appetite but dramatically improves the way your body processes stored fat and sugar, often with fewer nausea-related side effects.
- Generation 3: Triple-Receptor Agonists (GLP-1 + GIP + Glucagon). The absolute peak of current peptide engineering is Retatrutide. It activates three receptors. It keeps the fullness of GLP-1, the sugar-control of GIP, and adds the raw fat-burning, energy-boosting power of the Glucagon (GCG) receptor. This trio ramps up your base metabolic rate, essentially turning your body into a fat-burning furnace even when resting.
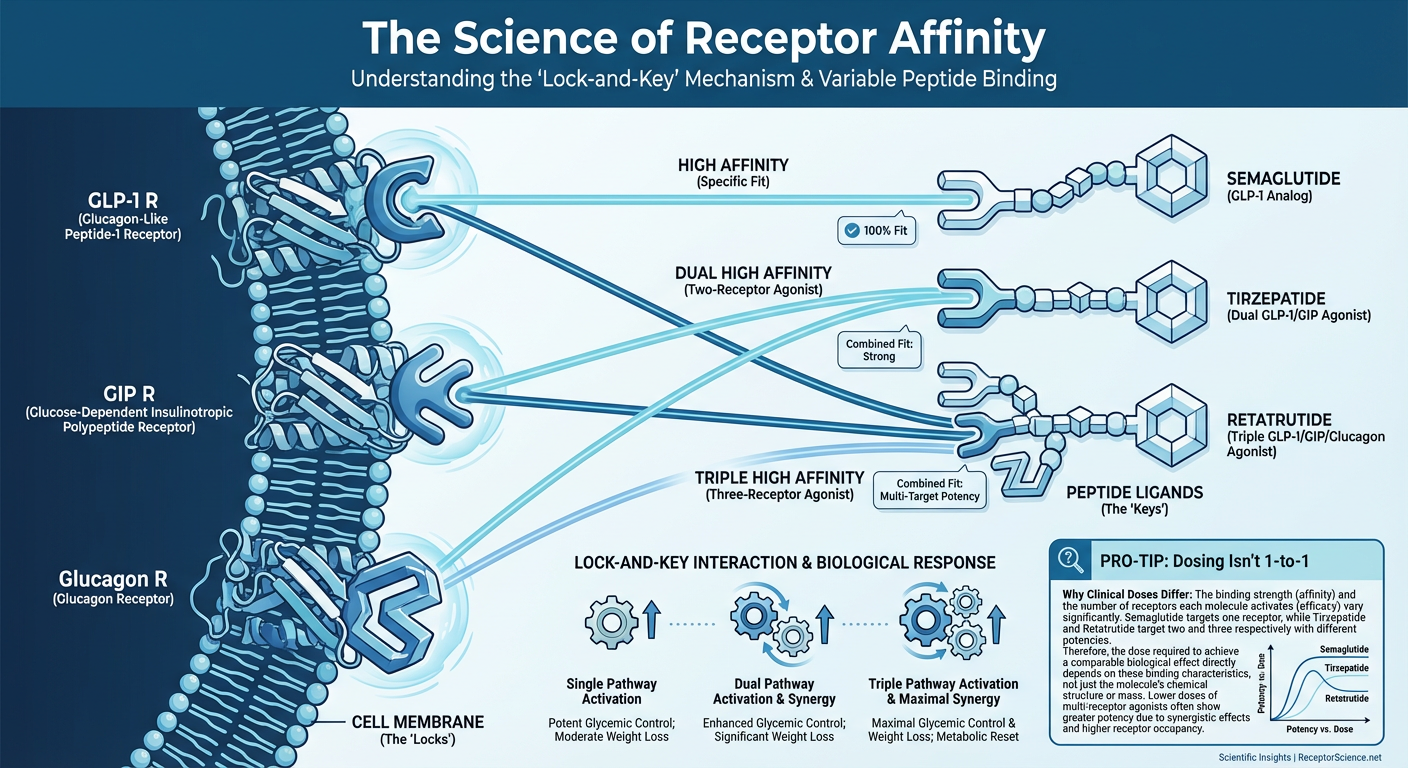
Understanding Receptor Affinity (The "Lock and Key" Mechanism)
Imagine your body's cells are covered in thousands of tiny doorways. To open a doorway and send a signal (like "burn fat" or "stop eating"), you need a specific key. Peptides are those keys.
In chemical terms, "affinity" describes how tightly and perfectly a peptide-key fits into a cellular-lock. If a peptide has a high affinity, it clicks into the lock instantly and holds on tight. You only need a very tiny dose to get massive results. If a peptide has a lower affinity for a certain lock, the key fits a bit looser. You might need a higher dose in milligrams to achieve an effect, but in return, you might experience a smoother, less abrupt biological response.
When scientists began making dual and triple agonists, they didn't just smash three full-strength keys together. If they had, the biological response would be overwhelming. Instead, brilliant researchers carefully "scaled" the affinity for each receptor.
For example, in a tri-agonist like Retatrutide, the peptide is designed to have a slightly altered affinity for the GLP-1 receptor compared to Semaglutide, balanced perfectly with its new GIP and Glucagon keys. This balance is exactly why you cannot use a straight milligram-to-milligram conversion when you switch from a first-generation protocol to a third-generation protocol. Let's break down the unique profiles of each powerhouse peptide.
The Foundation: Semaglutide (The Single Key)
Semaglutide is the name that brought peptide weight loss to the mainstream. As a pure GLP-1 receptor agonist, it focuses nearly all of its energy on one goal: unparalleled appetite suppression.
The affinity Semaglutide has for the GLP-1 receptor is incredibly high. Once injected, it binds tightly to receptors in the brain and gut. The gastric emptying process immediately slows down. If you eat a small meal, you feel as though you've just eaten Thanksgiving dinner. More importantly for many consumers, it creates a neurological quietness. That mid-afternoon craving for a sugary snack vanishes completely.
Typical Expectations & Dosing Curve
Because it only has one pathway, the strategy with Semaglutide is a steady, cautious upward climb. Researchers typically begin with a micro-dose of 0.25mg per week. Over several months, they titrate (gradually increase) up to a maximum dose of 2.4mg per week.
However, because Semaglutide binds so powerfully to the GLP-1 receptor without any other balancing hormones, some users experience nausea. The intense slowing of the gut can be uncomfortable if you eat large amounts of food or increase your dosage too quickly.
The Next Level: Tirzepatide (The Dual Engine)
When Tirzepatide hit the scene, it completely shifted the paradigm. Tirzepatide combines GLP-1 with a second incretin called GIP.
Here is where "receptor affinity" becomes wonderfully complex. Tirzepatide actively favors the GIP receptor. In fact, its binding affinity for GIP is essentially equal to your body's natural hormones, while its binding affinity for GLP-1 is actually lower than Semaglutide's. It sounds counterintuitive—why would a weaker key yield better results?
The answer is biological synergy. Because Tirzepatide utilizes the GIP pathway, it drastically improves insulin sensitivity and reduces fat accumulation fundamentally differently than GLP-1 alone. The GIP activation effectively "buffers" the intense nausea associated with strict GLP-1 agonism. Therefore, researchers can administer significantly higher overall milligram doses of Tirzepatide, yielding unprecedented fat loss results with remarkably tolerable side effects.
Molar Dosing and the Tirzepatide Transition
If you were to switch from Semaglutide to Tirzepatide, viewing the milligrams on the vial can be jarring. A max dose of Semaglutide is 2.4mg. A max dose of Tirzepatide is 15.0mg. This is what we mean by "comparative molar dosing." Tirzepatide is a larger, more complex molecule that requires a higher milligram volume to deliver its dual-action effect.
A transition requires starting lower on the new peptide to let the body adjust to the novel GIP stimulation, rather than assuming a high tolerance to GLP-1 means you can start at a maximum dose of Tirzepatide.
The Peak of Engineering: Retatrutide (The Tri-Agonist)
If Tirzepatide was a leap forward, Retatrutide is a rocket ship. Retatrutide is a single molecule that flawlessly activates GLP-1, GIP, and crucially, the Glucagon (GCG) receptor.
Why is Glucagon the holy grail for metabolic wellness? While GLP-1 and GIP primarily limit the calories you consume and how your body stores them, Glucagon actively forces your body to burn them. Glucagon goes aggressively after stored liver fat (visceral fat), pulling it out of the organs and converting it into usable energy. It significantly increases your resting energy expenditure. On Retatrutide, your body burns more calories just sitting on the couch than it would naturally.
Because Retatrutide includes Glucagon, the affinity balancing act is spectacular. Researchers optimized Retatrutide to prevent the "exhaustion" or plateau typical in long-term dieting. The Glucagon receptor provides a metabolic fire that pushes past standard GLP-1 plateaus.
Expectations on Retatrutide
Clinical data for Retatrutide shows mind-bending milestones. Study subjects have seen 24% or more of their total body weight vanish in under a year. Furthermore, the clearance of liver fat is so profound that many individuals see their cholesterol and triglyceride metrics optimize faster than with any previous protocol. It is currently the apex tool in the anti-obesity peptide arsenal.
Other Next-Generation Incretins on the Horizon
While Retatrutide dominates the current conversation, the landscape of multi-receptor peptides is rapidly expanding. For health innovators looking to customize their approach, several other brilliant compounds are emerging:
- Mazdutide: A unique dual-agonist targeting GLP-1 and Glucagon (skipping GIP). It is highly prized for scenarios where extreme mobilization of liver fat and rapid improvements in liver health are the primary goal alongside weight loss.
- Survodutide: Another GLP-1/Glucagon dual-agonist that has deliberately engineered very specific receptor affinities. It is showing massive promise not just in weight management, but in resolving severe liver inflammation conditions like MASH (Metabolic dysfunction-associated steatohepatitis).
- Cagrilintide: This isn't a traditional incretin; it's a long-acting amylin analogue. Amylin is a hormone co-secreted with insulin that delays gastric emptying and influences brain satiety centers entirely independently of GLP-1. Researchers are now stacking Cagrilintide with Semaglutide (often referred to as 'CagriSema') for a synergistic dual-pathway approach that bypasses GIP entirely.
The Mathematics of Transitioning: Comparing Dosages safely
When transitioning down the incretin pipeline—say, from Semaglutide to Tirzepatide, or from Tirzepatide to Retatrutide—understanding the math prevents unpleasant side effects and ensures a seamless transition of metabolic momentum.
Let's look at a comparative breakdown of how these peptides generally scale.
| Peptide | Receptor Targets | Starting Dose (Weekly) | Maximum Efficacy Dose (Weekly) | Primary Benefit Mechanism |
|---|---|---|---|---|
| Semaglutide | GLP-1 | 0.25 mg | 2.4 mg | Intense appetite suppression |
| Tirzepatide | GLP-1, GIP | 2.5 mg | 15.0 mg | Appetite control + Metabolic smoothing (Less nausea) |
| Retatrutide | GLP-1, GIP, GCG | 2.0 mg | 12.0 mg | Total appetite control + Active calorie burning (Thermogenesis) |
The "Washout" vs. The "Direct Switch"
If you've been using a maximum dose of 2.4mg Semaglutide, you cannot jump straight to 15.0mg of Tirzepatide, nor to 12.0mg of Retatrutide. Doing so introduces new hormone bindings (GIP and GCG) that your body hasn't adapted to.
From a technical standpoint, many researchers employ a "step-down, step-over" method. If replacing a maxed-out GLP-1 agonist, you might initiate the next-generation multi-agonist at its secondary or tertiary level (e.g., starting Tirzepatide at 5.0mg or 7.5mg, rather than the true baseline 2.5mg), because your GLP-1 receptors are already saturated and familiar with the signaling.
Conversely, if one is moving from Tirzepatide to Retatrutide, the introduction of the Glucagon receptor demands respect. The thermogenic (heat and energy producing) properties of Glucagon mean a lower starting threshold (often 2.0mg to 4.0mg) is necessary to accurately gauge heart rate and metabolic resting energy.
Real-World Results: What these Affinities Mean for YOU
What does this molecular magic translate to when you look in the mirror? The difference in receptor scaling radically changes the timeline and quality of your results.
- Shattering the Plateau: It is incredibly common for users on a single GLP-1 agonist to plateau after 6 to 9 months. The body adapts. By upgrading to a dual or tri-agonist, you introduce an entirely new metabolic signaling pathway. It essentially resets your body's "weight loss honeymoon phase."
- Better Energy Profiles: Single GLP-1s can sometimes cause lethargy. By slowing down gastric motility so significantly, and driving your caloric intake down, you might feel a bit sluggish. The dual and triple agonists—particularly those featuring Glucagon—actively compel the body to burn visceral fat for fuel, translating to massive spikes in sustained daily energy.
- Targeted Fat Loss vs. Total Weight Drop: Because multi-agonist compounds alter how insulin and glucagon interact, users frequently report superior body recomposition. You are not just stepping on the scale and seeing a lower number; you are seeing inches drop directly from the stubborn midsection as visceral lipid stores are forcefully mobilized.
Preserving Muscle During Extreme Weight Loss
With massive effectiveness comes a brand new challenge: muscle preservation. When peptides like Tirzepatide or Retatrutide successfully drop your body weight by 20% to 25%, you run the risk of losing lean muscle mass alongside the adipose tissue. This is commonly referred to in popular media as "Ozempic body" or premature facial aging.
A smart, well-rounded peptide protocol doesn't just address fat loss—it addresses aesthetic vitality and metabolic strength.
To counteract muscle wasting, intelligent researchers often supplement their incretin protocol with Growth Hormone Secretagogues (GHS). For instance, adding an evening protocol of Ipamorelin, paired occasionally with Tesamorelin, can be wildly effective. Tesamorelin is highly regarded for its ability to selectively target visceral adipose tissue while simultaneously releasing natural spurts of human growth hormone, protecting your hard-earned lean muscle.
Protecting lean muscle isn't just about vanity; muscle is highly metabolically active. The more muscle you retain during your weight-loss phase, the higher your basal metabolic rate remains, making it infinitely easier to maintain your new physique once you eventually taper off the incretins.
Quality Matters: Why Purity Impacts Potency and Dosage
We can discuss molar conversions and receptor affinities all day long, but if the compound you are utilizing is compromised, your results will be compromised as well.
Multi-receptor peptides are vastly more difficult to manufacture than single-receptor peptides. A tri-agonist like Retatrutide is a long, highly complex chain of amino acids subjected to meticulous modifications. If the synthesis is sloppy, the peptide may degrade rapidly, lose its affinity for the receptors, or cause harsh systemic inflammation.
At Alpha Carbon Labs, quality control is not a buzzword; it is an uncompromising standard. Producing these highly advanced molecules requires state-of-the-art peptide synthesis technology designed to eliminate toxic byproducts and stabilize the final compound. When comparing dosages, you must guarantee you are measuring pure, intact active pharmaceutical ingredients.
Never begin a sophisticated protocol without verifying third-party testing. Always look closely at the COA (Certificate of Analysis) documents. These documents ensure you receive the exact purity, mass, and sequence necessary for the biological response you are expecting.
Frequently Asked Questions (FAQ)
What exactly does "Comparative Molar Dosing" mean?
Because peptides have different molecular weights (their physical size and mass) and different receptor affinities, a milligram of one peptide does not equal a milligram of another. "Molar dosing" refers to scaling the dose based on the actual number of active molecules and how tightly they bind, rather than just raw scale weight. This is why 15mg of Tirzepatide is a normal dose, while 15mg of Semaglutide would be a massive, dangerous overdose.
Can I stack a GLP-1 like Semaglutide with a Tri-agonist like Retatrutide?
No, this is highly discouraged. Retatrutide already contains a perfectly engineered GLP-1 molecule within its structure. Stacking an additional, standalone GLP-1 peptide alongside a dual or tri-agonist will oversaturate the GLP-1 receptors. This leads directly to extreme nausea, gastrointestinal paralysis, and receptor downregulation without offering any additional weight-loss benefit.
Why does switching to a stronger peptide sometimes result in fewer side effects?
It comes down to natural synergy. First-generation peptides hammer one single receptor aggressively. This creates a bottleneck effect in your digestion. Dual and triple agonists utilize multiple pathways simultaneously. By spreading the metabolic signals across GLP-1, GIP, and Glucagon, they achieve a more balanced, harmonious effect mimicking your body's natural state, resulting in less concentrated gastrointestinal distress.
How do I combat the nausea while transitioning up?
The golden rules of incretin side-effect management include: Hydration (with ample electrolytes), eating frequent micro-meals instead of large portions, and focusing strictly on high-quality protein and complex fibers. Most importantly, give your body time to adjust to a new dosage level before increasing it again. Moving up too fast is the number one cause of compound intolerance.
Should I just start with Retatrutide if it is the strongest?
Not necessarily. For many people, a single or dual-agonist protocol provides all the metabolic push they need to reach their wellness goals. Retatrutide is best suited for individuals aiming for profound, extreme weight recomposition, or those who have successfully lost weight on other peptides but have hit a rigid plateau that lasts more than 8 weeks.
How does Glucagon prevent the "weight loss stall"?
When you lose significant body fat quickly via calorie restriction, your body's survival mechanisms kick in. Your resting metabolism drops in order to "save" energy, leading to a stall. Glucagon directly overrides this survival mechanism. It tells the body, "You have plenty of energy stored in liver and visceral fat—burn that right now." It elevates your baseline metabolic fires, breaking right through natural metabolic adaptation.
Moving Forward with Clarity
Scaling receptor affinities and transitioning between advanced incretins does not need to be a daunting task reserved only for endocrinologists. By understanding how GLP-1, GIP, and Glucagon receptors interact to squash appetite, refine insulin response, and burn raw fat, you can approach your body recomposition journey logically and safely.
Next-generation peptides like Tirzepatide and Retatrutide represent the absolute pinnacle of scientific bio-engineering. They offer health-conscious individuals tools previously thought impossible. Remember: respect the titration schedules, listen closely to your body's feedback, protect your lean muscle mass with complementary peptides, and above all, source your compounds from transparent, rigorously tested laboratories.
The science of weight loss has officially evolved. With the right strategy, your physique and metabolic health can evolve right alongside it.
References
- 1. Jastreboff, A. M., et al. (2023). Triple-Hormone-Receptor Agonist Retatrutide for Obesity—A Phase 2 Trial. The New England Journal of Medicine, 389(6), 514-526.
- 2. Jastreboff, A. M., et al. (2022). Tirzepatide Once Weekly for the Treatment of Obesity. The New England Journal of Medicine, 387(3), 205-216.
- 3. Wilding, J. P. H., et al. (2021). Once-Weekly Semaglutide in Adults with Overweight or Obesity. The New England Journal of Medicine, 384(11), 989-1002.
- 4. Coskun, T., et al. (2022). LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss. Cell Metabolism, 34(9), 1234-1247.e9.
- 5. Müller, T. D., et al. (2019). The incretin co-agonist project: A decade of progress. Cell Metabolism, 30(1), 16-20.
- 6. Finan, B., et al. (2015). Unimolecular Dual Incretins Maximize Metabolic Benefits in Rodents, Monkeys, and Humans. Science Translational Medicine, 5(209), 209ra151.
- 7. Habegger, K. M., et al. (2013). The metabolic actions of glucagon revisited. Nature Reviews Endocrinology, 9(12), 689-697.
- 8. Tschöp, M. H., et al. (2016). Unimolecular Polypharmacy for Treatment of Diabetes and Obesity. Cell Metabolism, 24(1), 51-62.
- 9. Urva, S., et al. (2022). The novel dual GIP and GLP-1 receptor agonist tirzepatide: clinical pharmacokinetics, pharmacodynamics, and cardiovascular safety. Clinical Pharmacokinetics, 61(10), 1417-1428.
- 10. Zimmerman, K. F., et al. (2023). Triple incretin agonists in the development of obesity treatments: looking beyond GLP-1. Current Opinion in Endocrinology, Diabetes and Obesity, 30(2), 121-127.
All research information is for educational purposes only. The statements made within this website have not been evaluated by the US Food and Drug Administration. The statements and the products of this company are not intended to diagnose, treat, cure or prevent any disease.