Tirzepatide and the Amylin Intersection: Investigating Synergistic Satiety in Multi-Incretin Research Models
Discover how combining Tirzepatide's GLP-1/GIP pathways with Amylin analogues like Cagrilintide creates synergistic satiety to break weight loss plateaus.
The Evolution of Weight Management: Beyond Willpower
For decades, the standard advice for weight loss was frustratingly simple: eat less, move more. Anyone who has ever been on a diet knows that this advice, while technically true on a thermodynamic level, entirely ignores the complex biology of the human body. When you try to restrict calories, your body fights back. It floods your system with hunger hormones, slows down your metabolism, and constantly whispers in your ear, urging you to seek out calorie-dense foods. This biological phenomenon, often referred to as "food noise," has been the downfall of millions of well-intentioned fitness journeys.
Fortunately, metabolic science has evolved past the era of pure willpower. We have entered the golden age of peptide therapies, where researchers are isolating the exact hormonal signals our bodies use to regulate hunger, energy, and fat storage. The first massive breakthrough in this space came with single-target peptides that activated the GLP-1 (Glucagon-Like Peptide-1) receptor. This single receptor activation changed the lives of countless individuals by signaling to the brain that the body was full.
But science never sleeps. Researchers soon realized that while targeting one receptor was good, targeting two was better. This realization brought us to a fascinating new intersection in metabolic optimization: the combination of powerful dual-agonists with entirely separate biological pathways. Today, we are diving deep into the science of synergistic satiety. We're looking at how Tirzepatide (a dual GLP-1 and GIP agonist) interacts with the Amylin pathway (often targeted by peptides like Cagrilintide) to create a multi-faceted approach to stubborn body fat, relentless cravings, and the dreaded weight loss plateau.
Whether you are on a journey to transform your physique, looking to optimize your health span, or simply searching for the most effective strategy to break through a wall in your weight loss journey, understanding this hormonal intersection is your front-row ticket to the future of metabolic wellness.
Understanding the Heavyweights: What is Tirzepatide?
Before we understand how these pathways work together, we need to understand the individual players in this metabolic symphony. The first major player is Tirzepatide. If older generations of weight management peptides were like targeting a problem with a sniper rifle, Tirzepatide is a highly coordinated synchronized drone strike.
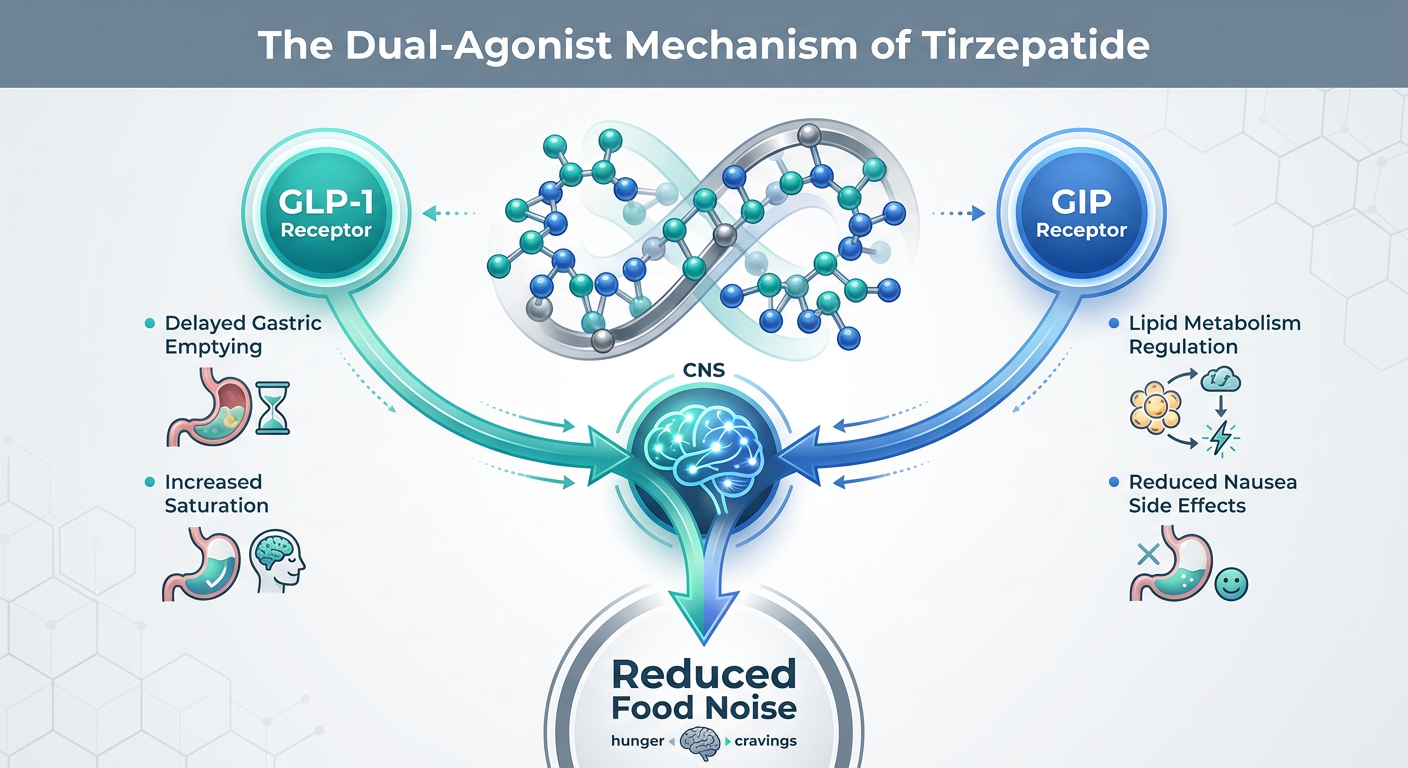
Tirzepatide is classified as a "dual-agonist." Unlike earlier molecules that only triggered the GLP-1 receptor, Tirzepatide activates two different, yet highly complementary, incretin hormone receptors in your body: GLP-1 (Glucagon-Like Peptide-1) and GIP (Glucose-Dependent Insulinotropic Polypeptide).
The Role of GLP-1
GLP-1 is a naturally occurring hormone produced in your gut when you eat. Its primary job is to tell your body, "Hey, food has arrived. Let's process it." It does this in two profound ways that aid in weight loss. First, it slows down gastric emptying—meaning the food you eat stays in your stomach significantly longer. This physically keeps you feeling full. Second, GLP-1 travels up to the hypothalamus in your brain, essentially switching off your appetite and muting the constant, nagging desire to snack.
The Role of GIP
GIP is the second half of this dynamic duo. Historically, researchers weren't sure if activating GIP would help or hinder weight loss. However, modern research has shown that when combined with GLP-1, GIP is an absolute powerhouse. GIP receptors are found heavily throughout adipose (fat) tissue and the brain. GIP helps regulate how your body stores and utilizes fat, improves the sensitivity of your cells to insulin, and further suppresses appetite. Furthermore, it appears to reduce some of the nausea typically associated with pure GLP-1 activation.
By activating both GLP-1 and GIP naturally produced signals, Tirzepatide instructs the body to efficiently manage blood sugar, stop craving extra calories, and begin utilizing stored body fat for energy. It was a revolutionary leap forward, setting records in clinical studies for overall fat reduction. But for some individuals, even the power of two receptors isn't enough to reach their ultimate health goals.
Enter Amylin: The Missing Satiety Hormone
If GLP-1 and GIP are the dynamic duo of metabolic health, Amylin is the secret mastermind operating behind the scenes. Amylin is a hormone co-secreted with insulin by the beta cells of your pancreas. Every time you eat a meal and your body releases insulin to manage the incoming energy, it also pumps out Amylin. For decades, Amylin lived in insulin's shadow, vastly under-appreciated by the fitness and wellness communities.
So, what exactly does Amylin do? In simple terms, it is a potent "satiety signal." Like GLP-1, it slows down the rate at which food empties from your stomach into your small intestine. However, Amylin’s real superpower lies in how it communicates with your brain.
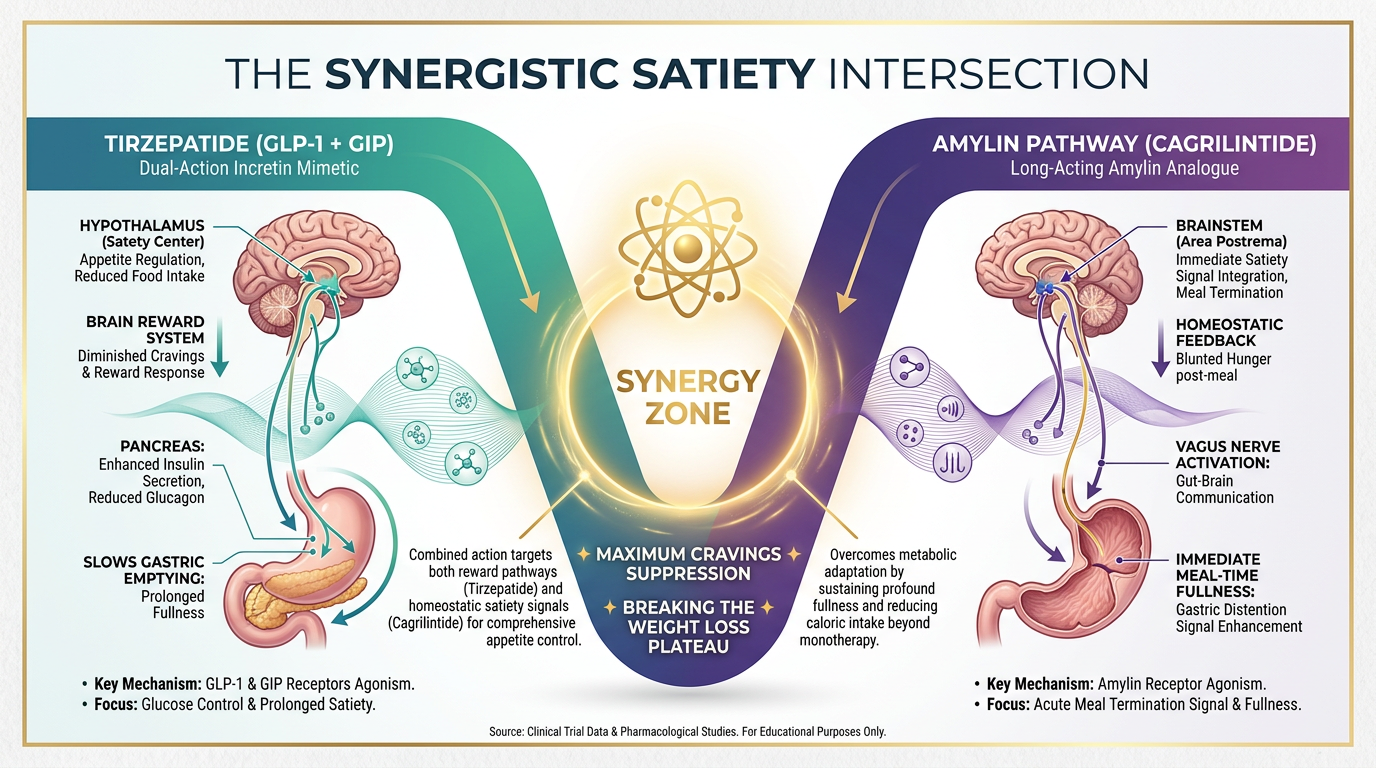
While GLP-1 primarily communicates with the hypothalamus (the control center for hunger and energy balance), Amylin targets a completely different area of the brain: the hindbrain (specifically, the area postrema). This is an incredibly important distinction. The hindbrain serves as a major sensory relay station. When Amylin hits the hindbrain, it triggers an immediate and robust sensation of "meal-ending fullness." We call this satiation.
To put it in everyday terms: GLP-1 helps you feel less hungry between meals (satiety), while Amylin helps you feel incredibly full *during* the meal so you stop eating sooner (satiation). When you combine these two signals, the amount of food required to feel comfortably full plummets.
Cagrilintide: The Modern Amylin Analogue
Because natural Amylin disappears from the bloodstream very quickly, researchers needed to create a synthetic version that lasted longer. This is where Cagrilintide comes into the picture. Cagrilintide is a long-acting Amylin analogue (a man-made molecule designed to mimic natural Amylin) that typically lasts for about a week in the body.
On its own, Cagrilintide has shown profound promise in metabolic studies, causing significant weight reduction purely by forcing the brain to recognize fullness through the hindbrain pathway. However, researchers quickly realized a fundamental truth of human biology: the body is incredibly adaptable. If you only suppress appetite through one pathway (just Amylin, or just GLP-1), the body will eventually try to compensate and sneak cravings back in. To truly outsmart the body's natural drive to hold onto fat, you need to trigger multiple pathways at the exact same time.
The Science of Synergistic Satiety: Connecting the Pathways
The term "synergy" is often thrown around as a buzzword, but in endocrinology and peptide science, it has a very specific meaning. Synergy means that the combined effect of two compounds is greater than the sum of their individual parts. Let's say Peptide A gives you a metabolic boost of 2, and Peptide B gives you a metabolic boost of 2. Additive results would equal 4. Synergistic results equal 6, 8, or even 10.
When you combine incretin therapy (GLP-1/GIP) with Amylin therapy, you are creating the ultimate environment for synergistic satiety. Here is exactly why hitting these combined intersections is viewed as the holy grail of metabolic control:
- Dual Brain-Targeting: As mentioned, GLP-1 targets the hypothalamus to reduce food cravings and "food noise," while Amylin targets the hindbrain to promote immediate physical fullness. By stimulating both centers simultaneously, the brain receives an overwhelming, undeniable message that the body is nourished and requires zero excess calories.
- Enhanced Gastric Control: Both pathways naturally act to slow gastric emptying. Together, they create a highly regulated digestive pace. Slowing down digestion prevents post-meal blood sugar spikes, which are the primary culprits behind sudden energy crashes and intense sugar cravings later in the day.
- Fat-Burning Amplification: With the GLP-1/Amylin pathways effectively shutting down caloric intake effortlessly, the GIP pathway from a molecule like Tirzepatide is free to shine. GIP activity improves fat metabolism at the cellular level, helping the body recognize that it's okay to crack open those stubborn fat stores (like love handles or belly fat) for energy.
For a consumer trying to get lean, look younger naturally, and optimize their physique, synergistic satiety means the journey stops feeling like an uphill battle. You no longer have to grip the steering wheel white-knuckled, fighting off the urge to eat a late-night snack. Your biology simply handles it for you.
Breaking the Dreaded Weight Loss Plateau
Perhaps the most prevalent, frustrating, and demoralizing part of any fitness journey is the weight loss plateau. You do everything right. You eat wholesome foods, prioritize your protein, lift weights, and use a premium peptide like Semaglutide or Tirzepatide. For months, the results are magical. The fat melts away.
And then... it stops. Week after week, the scale refuses to budge. The cravings that disappeared six months ago slowly start to creep back into your mind. Why does this happen?
It happens because your biology is specifically evolved to prevent you from starving. This is known as the "set point theory" or "metabolic adaptation." When you lose a significant amount of weight, your body senses a threat. In response, it down-regulates your metabolism, lowers your daily energy expenditure, and ramps up hunger hormones like ghrelin trying to force you to return to your previous weight. Eventually, the power of a single or even dual-receptor peptide may be evenly matched by your body's defensive hunger signals.
Outsmarting Adaptation with the Amylin Pathway
This is precisely where the Amylin intersection steps in to save the day. When an individual hits a hard plateau on GLP-1 therapies, introducing an Amylin analogue introduces a completely novel, un-adapted signal to the brain. Because the brain hasn't built up a tolerance to robust Amylin signaling, hitting that hindbrain receptor breaks through the plateau like a battering ram.
Research models heavily suggest that by stacking mechanisms—activating GIP, GLP-1, and Amylin simultaneously—metabolic adaptation can be successfully bypassed. The body's biological defense mechanisms simply cannot out-signal the combined strength of these three satiation pathways.
Comparing the Stacks: CagriSema vs. Tirzepatide and Amylin
To fully grasp this intersection, it's helpful to look at how these combinations are put into practice in research models. Currently, the most well-documented multi-pathway combination involving Amylin is the combination of Cagrilintide and Semaglutide, often studied under the moniker CagriSema.
Let's take a look at the Cagrilintide + Semaglutide Blend and compare it theoretically with the Tirzepatide + Amylin concept in the chart below.
| Feature | Tirzepatide (Monotherapy) | Cagrilintide + Semaglutide Blend (Dual Pathway) | Tirzepatide + Amylin Analogue (Triple Pathway) |
|---|---|---|---|
| Receptors Targeted | GLP-1 and GIP | GLP-1 and Amylin | GLP-1, GIP, and Amylin |
| Primary Brain Target | Hypothalamus | Hypothalamus & Hindbrain | Hypothalamus & Hindbrain |
| Satiety Profile | Excellent craving control | Profound physical fullness | Maximum synergistic satiation; unyielding appetite control |
| Fat Metabolism | High (driven by GIP activity) | Moderate (driven by profound calorie deficit) | Extreme (highest fat utilization + ultimate calorie restriction) |
| Best Use Case | General, steady weight loss, excellent for initial phases. | Breaking Semaglutide plateaus, aggressive craving reduction. | Theoretical "nuclear option" for profound, stubborn metabolic resistance. |
The Cagrilintide + Semaglutide blend is already viewed as a highly advanced iteration of metabolic care. But the frontier of science is now asking: if Semaglutide and Cagrilintide are phenomenal together, what happens when we substitute Semaglutide for the even more powerful Tirzepatide? Connecting the Amylin pathway to GIP and GLP-1 represents the absolute cutting-edge of fat-loss optimization.
Maximizing Results on Multi-Pathway Therapies
While peptides are incredibly powerful, they are not magic wands. Think of them as the ultimate engine for your car—you still need to supply the right fuel and steering to win the race. To truly benefit from "synergistic satiety," you must align your lifestyle with your biochemistry.
1. Prioritize High-Quality Protein
When you are combining powerful appetite suppressants like Tirzepatide and an Amylin analogue, you are going to eat drastically less. Satiety will set in incredibly fast. Because your overall food volume is low, every single bite matters. To protect your lean muscle mass and support anti-aging, prioritize lean protein (chicken, fish, eggs, high-quality plant proteins) above all else. Aim for at least 0.8 to 1 gram of protein per pound of lean body mass. Protein also has a high thermic effect, meaning your body burns calories just digesting it!
2. Engage in Resistance Training
Weight loss is great, but fat loss is the true goal. If you want to look toned, youthful, and strong, you must signal to your body that your muscles are necessary for survival. Lifting weights (or doing bodyweight exercises like push-ups and squats) two to three times a week tells your central nervous system to hold onto precious muscle tissue while the peptides force your body to burn pure fat for energy.
3. Explore Synergistic Metabolic Peptides
For individuals looking to go above and beyond, managing body composition while in a deep calorie deficit can be supported by other fascinating metabolic peptides. For example, 5-Amino-1MQ is highly researched for its ability to target the NNMT enzyme in fat cells, actively encouraging cellular energy expenditure and helping shrink fat cells from a completely different non-hormonal angle. Combining an appetite pathway manipulator with a cellular energy optimizer is a hallmark of advanced research models.
4. Stay Hydrated and Manage Electrolytes
Given the slower gastric emptying associated with GLP-1 and Amylin agonists, thirst signals can sometimes become muted. Furthermore, as your body sheds glycogen (stored carbohydrates) during the initial phases of weight loss, it flushes out significant water and electrolytes. Be proactive. Drink plenty of water and consider adding a high-quality, sugar-free electrolyte supplement to prevent fatigue and headaches.
The Future of Multi-Incretin Therapy: Looking Toward Retatrutide
As we analyze the synergy of Tirzepatide and Amylin, it’s impossible to ignore the future landscape of multi-receptor peptides. The next giant leap currently dominating clinical trials is Retatrutide. Retatrutide is a "triple agonist" that targets GLP-1, GIP, and a third receptor: Glucagon.
How does this compare to adding Amylin? It comes down to mechanism of action.
- Retatrutide (GLP-1 + GIP + Glucagon): Focuses heavily on increasing base metabolic rate. The glucagon receptor activation specifically tells the liver to burn more energy and fat. It attacks weight loss by spiking your daily calorie burn while managing appetite.
- Tirzepatide + Amylin Strategy: Focuses primarily on overwhelming the body’s satiety centers. It attacks weight loss by creating a biological environment where overeating becomes nearly impossible and cravings are rendered virtually non-existent, while the GIP still supports fat metabolism.
Both pathways represent the pinnacle of metabolic science. Which pathway is "better" ultimately depends on an individual's specific biological hurdles—whether they struggle more with a sluggish metabolism (leaning toward Retatrutide) or insatiable hunger (leaning toward intense Amylin combinations).
The Crucial Importance of Quality, Purity, and Trust
When exploring advanced peptide therapies and complex molecular interactions, nothing is more critical than the purity of the compounds. The sophisticated biological signaling we've discussed—the precise communication between your gut, your hindbrain, and your fat cells—requires perfectly sequenced, pure peptides.
At Alpha Carbon Labs, we recognize that our community demands excellence. We invite our customers to look "under the hood" at our commitment to unparalleled purity. Exploring advanced mechanisms is only viable when backed by stringent quality control standards.
Every batch undergoes highly localized, meticulous advanced peptide synthesis to ensure sequence accuracy. Furthermore, we proudly provide verifiable COA (Certificate of Analysis) documents for our entire catalog. A COA acts as a scientific receipt, provided by highly credible third-party laboratories, confirming that the molecule you are researching is exactly what we say it is—free from contaminants, heavy metals, or degraded by-products. If you want a synergistic, clinical-grade result, you must use clinical-grade tools.
Frequently Asked Questions
Can you stack GLP-1 therapies with Amylin peptides?
Yes, in both research and clinical settings, the combination of GLP-1 therapies and Amylin analogues is highly popular and well-documented. Because they target completely entirely different receptors and distinct parts of the brain (the hypothalamus and the hindbrain), they don't compete with one another. Instead, they work harmoniously to quiet the mind's desire for food and drastically reduce the physical volume of food required to feel full. The blended approach often helps individuals who have become resistant to standard monotherapies.
How quickly does synergistic satiety take effect?
Individuals researching Amylin analogues alongside GLP-1/GIP molecules routinely report an almost immediate change in appetite on the days following administration. Because the hindbrain responds rapidly to Amylin signals, the sensation of early fullness during meals happens very quickly. Sustained weight and fat loss, however, require weeks and months of compounding, consistent caloric deficit, and improved metabolic function mediated by the GIP pathways.
What happens to my muscle mass while losing weight this way?
Muscle loss is a risk during *any* period of rapid weight reduction, regardless of whether it is mediated by peptides, fasting, or gastric bypass surgery. Because the Tirzepatide and Amylin combination reduces appetite so heavily, it's vital to eat strategically. Consume high protein (prioritizing it first on the plate) and stimulate the muscle through weight training. The body is an efficient machine; it won't break down muscle tissue for energy if you constantly signal that the muscle is actively in use.
Will I feel nauseous by combining these peptides?
Because both GLP-1 and Amylin slow down gastric emptying, rapid dose escalation can indeed lead to feelings of fullness that quickly cross the line into nausea or indigestion. Gastric distress is usually a sign that food is sitting in the stomach for too long without moving. The most successful approach into multi-receptor therapy is a philosophy of "start low and go slow." Allow the digestive tract to acclimate to its new, slower pace before pushing up to higher combinations.
When should I consider stepping up from a single peptide to a combination?
Most experts suggest utilizing a single-pathway or dual-pathway peptide (like Semaglutide or Tirzepatide alone) until you hit a true, unbreakable plateau. A plateau is generally defined as no changes on the scale or in body measurements for 4–6 weeks despite strict adherence to diet and exercise. Once metabolic adaptation has stalled progress, introducing the missing Amylin signal is an excellent strategic maneuver to restart the fat-burning furnace.
Conclusion
We are living through a renaissance in metabolic health. The days of fighting a losing battle against your own biology, feeling constantly hungry, and suffering through yo-yo diet cycles are coming to an end. By understanding and utilizing the synergistic satiety created by combining Tirzepatide's GLP-1 and GIP signaling with the powerful, brain-targeting pathway of Amylin, you open the door to unprecedented weight loss and bodily optimization. Remember to pair these cutting-edge research tools with a high-protein diet, sensible lifestyle modifications, and an unwavering commitment to pure, top-tier quality compounds. Achieve the vitality, body composition, and longevity you deserve.
References
- 1. Jastreboff, A. M., Aronne, L. J., Ahmad, N. N., Wharton, S., Connery, L., Alves, B., ... & Stefanski, A. (2022). Tirzepatide once weekly for the treatment of obesity. New England Journal of Medicine, 387(3), 205-216.
- 2. Lau, D. C., Erichsen, L., Francisco, A. M., Satylganova, A., le Roux, C. W., McGowan, B., ... & Pedersen, S. D. (2021). Once-weekly cagrilintide for weight management in people with overweight and obesity: a multicentre, randomised, double-blind, placebo-controlled and active-controlled, dose-finding phase 2 trial. The Lancet, 398(10317), 2160-2172.
- 3. Enebo, M. I., Kruse, E. K., Kvist, K., Nørgaard, O. T., Olesen, J. N., Overgaard, R. V., ... & Clemmensen, B. O. (2023). Cagrilintide plus semaglutide for weight management in people with overweight and obesity (CagriSema): a randomised, double-blind, placebo-controlled, phase 2 trial. The Lancet, 401(10378), 1269-1278.
- 4. Finan, B., Ma, T., Ottaway, N., Muller, T. D., Habegger, K. M., Heppner, K. M., ... & DiMarchi, R. D. (2013). Unimolecular dual incretins maximize metabolic benefits in rodents, monkeys, and humans. Science Translational Medicine, 5(209), 209ra151.
- 5. Boyle, C. N., Lutz, T. A., & Le Foll, C. (2018). The role of amylin in systemic metabolism and body weight regulation. Physiology & Behavior, 192, 97-105.
- 6. Chao, A. M., Jastreboff, A. M., White, M. A., Grilo, C. M., & Sinha, R. (2023). Food craving, food reward, and food intake in obesity and weight management. Current Obesity Reports, 1-13.
- 7. DeBlock, C. E., Van Gaal, L. F., & Scheen, A. J. (2022). Co-agonist treatments for obesity: The next generation of therapies. Trends in Endocrinology & Metabolism, 33(4), 282-297.
- 8. Samms, R. J., Coghlan, M. P., & Sloop, K. W. (2021). Gastric inhibitory polypeptide (GIP) receptor agonism mediates weight loss via centrally mediated reductions in food intake and energy expenditure. Nature Metabolism, 3(1), 123-134.
- 9. Neary, N. M., Goldstone, A. P., & Bloom, S. R. (2004). Appetite regulation: from the gut to the hypothalamus. Clinical Endocrinology, 60(2), 153-160.
- 10. MacLean, P. S., Bergouignan, A., Cornier, M. A., & Jackman, M. R. (2011). Biology's response to dieting: the impetus for weight regain. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 301(3), R581-R600.
All research information is for educational purposes only. The statements made within this website have not been evaluated by the US Food and Drug Administration. The statements and the products of this company are not intended to diagnose, treat, cure or prevent any disease.