Peripheral Nerve Regeneration: The Synergistic Potential of ARA-290 and BPC-157 in Neuropathic Research
Discover how combining ARA-290 and BPC-157 can accelerate peripheral nerve regeneration. Learn about the science of the Innate Repair Receptor (IRR) and how this peptide stack targets nerve pain and healing.
Peripheral Nerve Regeneration: The Synergistic Potential of ARA-290 and BPC-157 in Neuropathic Research
If you have ever experienced the burning, tingling, or numbing sensation of nerve damage, you know that "pain" is an understatement. Unlike a simple cut or a bruise that heals visibly over a week, nerve damage (neuropathy) often feels like a silent, invisible battle. It’s a glitch in your body’s electrical wiring system that conventional medicine struggles to fix.
For years, the standard approach to neuropathy has been management, not repair. Doctors prescribe medications to dull the signals—essentially turning down the volume on the radio without fixing the broken antenna. But what if we could actually repair the wire?
This is where the frontier of peptide research is changing the game. Specifically, two compounds are making waves for their ability to not just mask pain, but to actively encourage the body to repair damaged neural tissue: ARA-290 and BPC-157.
While BPC-157 is widely known in the fitness world for healing tendons and gut issues, its role in nerve repair is equally profound. When combined with ARA-290, a peptide specifically engineered to target inflammation and nerve regeneration, we see a potential "synergy" that could redefine how we look at healing. Let’s dive into the science of this powerful duo and how they target the body's hidden "repair switch"—the Innate Repair Receptor.
The Problem with Nerves: Why They Are So Hard to Heal
To understand why these peptides are so special, we first have to respect the complexity of the nervous system. Your peripheral nerves are fragile, intricate communication lines that run from your spinal cord to the tips of your fingers and toes. When they are damaged—whether by high blood sugar (diabetes), physical trauma, autoimmune attacks, or compression—they don't just "snap back" like a rubber band.
Nerves regenerate incredibly slowly. Under perfect conditions, a nerve might regrow at a rate of 1 millimeter per day. But conditions are rarely perfect. Chronic inflammation, poor blood flow, and scar tissue often create a hostile environment that halts this regeneration entirely. This leaves the nerve stuck in a state of dysfunction, constantly misfiring pain signals or failing to transmit touch sensations.
This is where our two research subjects come in. They don't just hope for the best; they actively engineer a better environment for healing.
Meet the Specialist: ARA-290
If you are looking for a precision tool designed for nerve health, ARA-290 is it. To understand ARA-290, we have to look at a hormone you might already know: Erythropoietin, or EPO.
EPO is famous in the sports world for boosting red blood cell production. However, scientists discovered that EPO also has powerful tissue-protective effects. The problem? You can't just give someone massive doses of EPO for nerve pain because it would thicken their blood to dangerous levels. Scientists needed the healing benefits of EPO without the red blood cell stimulation.
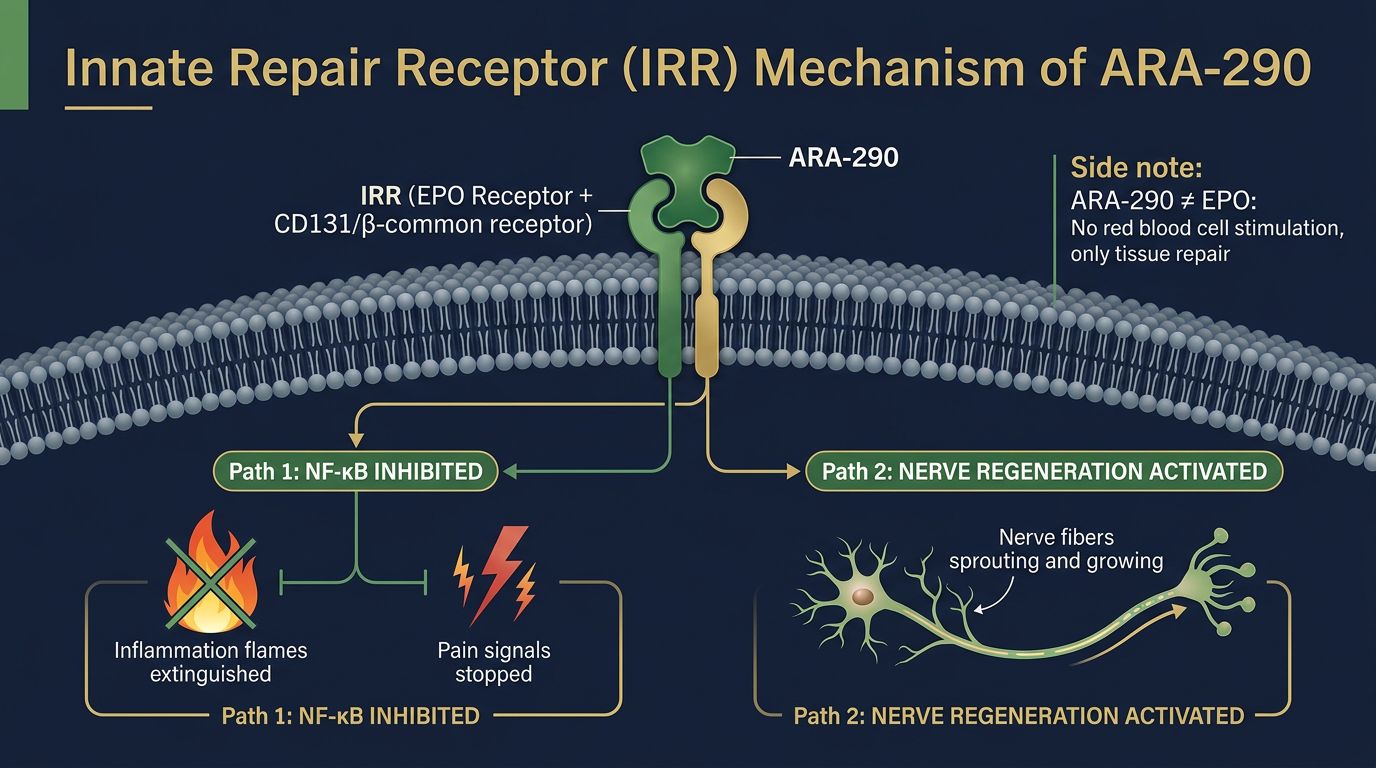
Enter ARA-290. This peptide is a synthetic fragment of EPO designed to trigger the body's repair mechanisms without affecting red blood cells. It works by activating a specific receptor known as the Innate Repair Receptor (IRR).
What is the Innate Repair Receptor (IRR)?
Think of the IRR as a "Master Switch" for healing that exists on the surface of cells, particularly immune cells and nerve cells. In a healthy, calm body, this switch is off. But when tissues are damaged or stressed, the body presents the IRR receptor, waiting for a signal to turn on the repair crew.
When ARA-290 binds to the IRR, it does two critical things:
- It shuts down inflammation: It tells the immune system to stop attacking the damaged area, switching the focus from "defense" to "reconstruction."
- It stimulates regeneration: It promotes the sprouting of small nerve fibers, which are often the first to die in conditions like Small Fiber Neuropathy (SFN).
Meet the General: BPC-157
While ARA-290 is the sniper targeting the nerve switch, BPC-157 is the army corps of engineers building the infrastructure. Known as the "Body Protection Compound," BPC-157 is a pentadecapeptide derived from human gastric juice.
Why is a stomach peptide good for nerves? Because BPC-157 is the ultimate systemic healer. Its primary superpower is angiogenesis—the formation of new blood vessels. Nerves are incredibly hungry tissues; they require a robust supply of oxygen and nutrients to function and repair. If the blood supply is poor (a common issue in diabetic neuropathy), the nerve starves and dies.
BPC-157 works by:
- Restoring Blood Flow: It creates new distinct pathways for blood to reach damaged tissues, ensuring the nerves have the fuel they need to regrow.
- Protecting the Myelin Sheath: Research suggests BPC-157 can help protect and repair the insulating layer around nerves, ensuring signals travel fast and true.
- Modulating Fibrosis: It prevents excessive scar tissue formation, which can trap nerves and prevent them from reconnecting.
The Synergy: How ARA-290 and BPC-157 Work Together
In the world of peptide research, stacking (combining) peptides is done to cover multiple pathways of healing simultaneously. The combination of ARA-290 and BPC-157 is becoming a gold standard for neuropathic research because they address the two biggest hurdles in nerve regeneration: inflammation and nutritional supply.
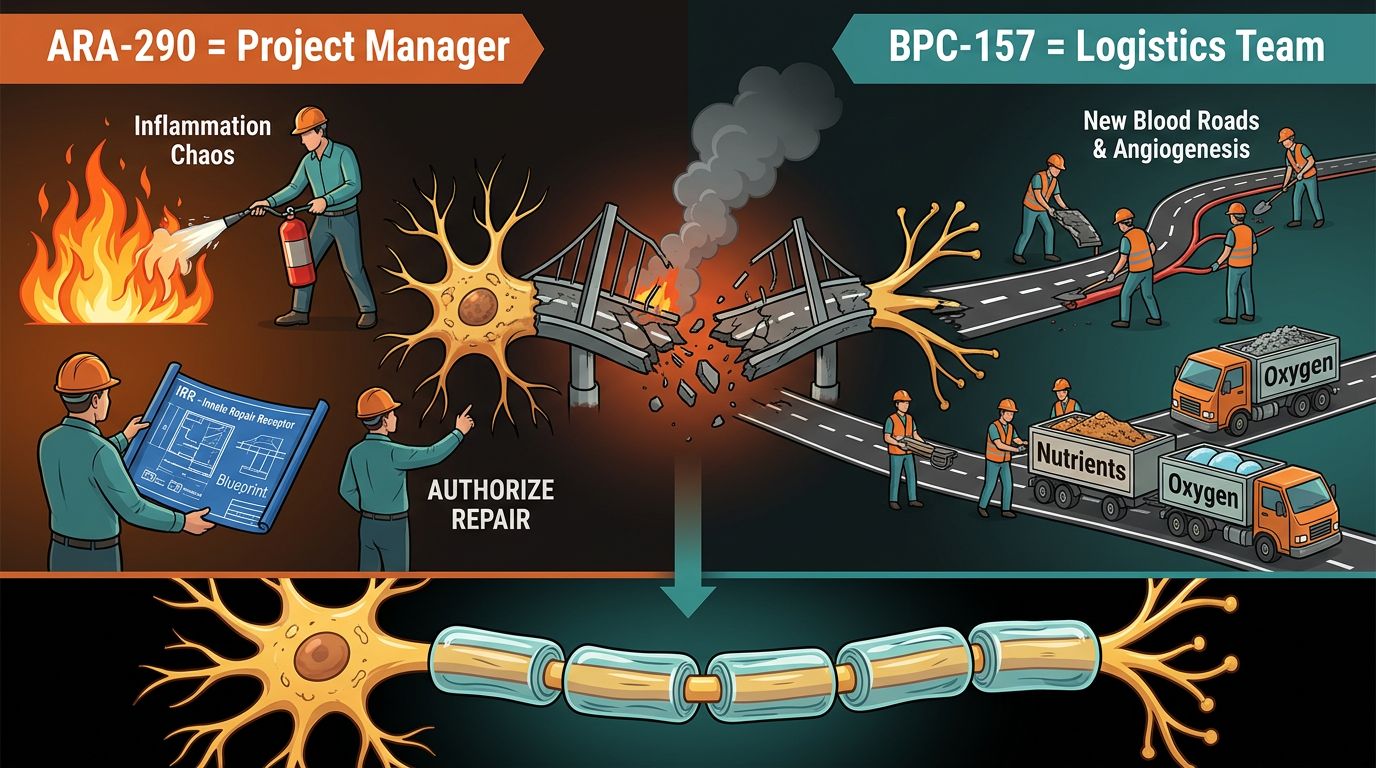
The "Construction Site" Analogy
Imagine your damaged nerve is a collapsed bridge.
- ARA-290 is the project manager who arrives on the scene, calms the panic (inflammation), and authorizes the blueprints for the new bridge (activates the IRR). Without it, the workers just stand around confused.
- BPC-157 is the logistics team that builds the roads to the site (blood vessels) and trucks in the cement and steel (nutrients). Without it, the project manager has no materials to build with.
By using them together, you create a "pro-healing" environment where the instructions are clear (ARA-290) and the resources are plentiful (BPC-157). This synergistic effect is why many researchers believe the combination is far superior to using either peptide in isolation for complex nerve damage.
Deep Dive: The Science of the "Innate Repair Receptor"
We mentioned the IRR earlier, but it deserves a closer look because it is the cornerstone of why this protocol works. The discovery of the Innate Repair Receptor turned our understanding of inflammation on its head.
The IRR is a heteroreceptor complex formed by the erythropoietin receptor and the beta-common receptor (CD131). It is essentially a safety valve for the body. During chronic disease or injury, inflammatory cytokines (bad signals) flood the system, causing pain and further tissue destruction. This is "sterile inflammation"—it serves no purpose other than to cause suffering.
When ARA-290 activates the IRR, it inhibits the nuclear factor-kappa B (NF-κB) pathway. If you aren't a molecular biologist, that sounds like gibberish. In plain English: It turns off the gene that produces pain and inflammation.
This is crucial for neuropathy because neuropathic pain is often maintained by a vicious cycle of inflammation. The nerve gets hurt, it gets inflamed, the inflammation hurts the nerve more, and the cycle repeats. ARA-290 breaks this cycle, silencing the "alarm" so the body can finally hear the "repair" orders.
Real-World Applications: What Are People Researching?
While we cannot make medical claims, we can look at the published literature and anecdotal reports from the biohacking community to see where this stack is showing promise.
1. Small Fiber Neuropathy (SFN)
SFN is notoriously difficult to diagnose and treat. It affects the tiny nerve endings in the skin and organs, causing burning pain, heart palpitations, and digestive issues. Research specifically on ARA-290 has shown it can increase the density of these small nerve fibers in the cornea of the eye and the skin, correlating with reduced pain scores. Adding BPC-157 may support the vascular health of these tiny fibers.
2. Diabetic Neuropathy
High blood sugar acts like shards of glass in the blood vessels, shredding the capillaries that feed the nerves. This leads to the classic numb/painful feet of diabetes. BPC-157’s ability to promote angiogenesis is vital here, potentially restoring blood flow to these starving nerves, while ARA-290 combats the systemic inflammation caused by the metabolic disease.
3. Post-Surgical Recovery
Surgery inevitably cuts through nerves. Numbness or "phantom pains" around scars are common. Applying this peptide stack in a research setting aims to accelerate the re-innervation of the tissue, potentially reducing post-operative recovery times and preventing chronic pain from setting in.
4. Sciatica and Impingement
When a disc bulges in your back and crushes the sciatic nerve, the damage is twofold: mechanical pressure and chemical inflammation. Even after the pressure is removed (via surgery or therapy), the nerve remains inflamed. This stack targets that lingering inflammation.
How Does This Compare to Other Peptides?
There are many healing peptides out there. How does the ARA-290 + BPC-157 stack measure up against others? Let’s compare.
| Peptide | Primary Mechanism | Best For |
|---|---|---|
| ARA-290 | Activates Innate Repair Receptor (IRR); anti-inflammatory. | Nerve pain, small fiber neuropathy, autoimmune inflammation. |
| BPC-157 | Angiogenesis (blood vessel growth); fibroblast modulation. | Tendons, ligaments, gut health, general tissue support. |
| TB-500 | Actin upregulation (cell mobility). | Muscle recovery, flexibility, reducing scar tissue. |
| GHK-Cu | Copper transport; collagen synthesis; anti-oxidant. | Skin quality, cosmetic healing, mild nerve support. |
While compounds like TB-500 are excellent for muscle and large tissue injuries, they lack the specific neuro-protective mechanism of ARA-290. GHK-Cu is fantastic for skin, but for deep nerve repair, the ARA/BPC combo is currently the heavyweight champion in the research community.
Enhancing the Stack: Ancillary Compounds
For those looking to optimize their research even further, there are other compounds that play nice with ARA-290 and BPC-157.
TB-500 (Thymosin Beta-4)
If the injury involves muscle trauma alongside nerve damage (common in carpal tunnel or sports injuries), adding TB-500 can be beneficial. TB-500 helps cells migrate to the site of injury. If BPC-157 builds the road, TB-500 is the bus that drives the workers to the site.
GHK-Cu (Copper Peptide)
Copper is essential for the function of enzymes involved in nerve maintenance. GHK-Cu has been shown to reset genes to a younger, healthier state. In a topical application or systemic review, it supports the overall environment of the skin and superficial nerves.
Research Protocols: Dosing and Duration
Disclaimer: The following is based on typical research study parameters and is for informational purposes only. Alpha Carbon Labs provides peptides for research purposes, not for human consumption.
In successful studies involving ARA-290, consistency is key. Because nerves heal slowly, researchers often look at timelines of 4 to 12 weeks to see significant changes in nerve density.
- ARA-290: Often researched at dosages of 4mg per administration. Because it has a short half-life, daily administration is common in literature to keep the IRR activated periodically.
- BPC-157: Typically researched at 250mcg to 500mcg daily or twice daily. The systemic nature of BPC-157 means it is effective regardless of the injection site, though proximity to the injury is often preferred in animal models.
The "Synergy Protocol" typically involves administering both compounds daily. Some researchers mix them, while others administer them separately to observe distinct effects.
The Importance of Purity in Nerve Research
When dealing with the nervous system, purity is non-negotiable. Nerves are hypersensitive. Introducing impurities, heavy metals, or degradation byproducts into a research subject can cause inflammation—the exact opposite of what you are trying to achieve.
Low-quality peptides often contain endotoxins. If you inject an endotoxin into an area with nerve damage, you can trigger a massive immune response that sets healing back by weeks. This is why sourcing from a transparent, verified supplier is critical.
At Alpha Carbon Labs, we adhere to strict verification standards:
- HPLC Purity: We ensure our peptides are at least 99% pure.
- Mass Spectrometry: verifies the correct molecular weight and sequence.
- Third-Party Testing: We don't just say it; we prove it. You can view our COA Documents for every batch.
You can learn more about our rigorous testing process on our Quality Control page or read about how we manufacture these compounds in our section on peptide synthesis.
What to Expect: Timelines for Nerve Repair
If you are researching these peptides, patience is the most important variable. Unlike muscle tissue, which turns over rapidly, neural tissue acts on a geological timescale.
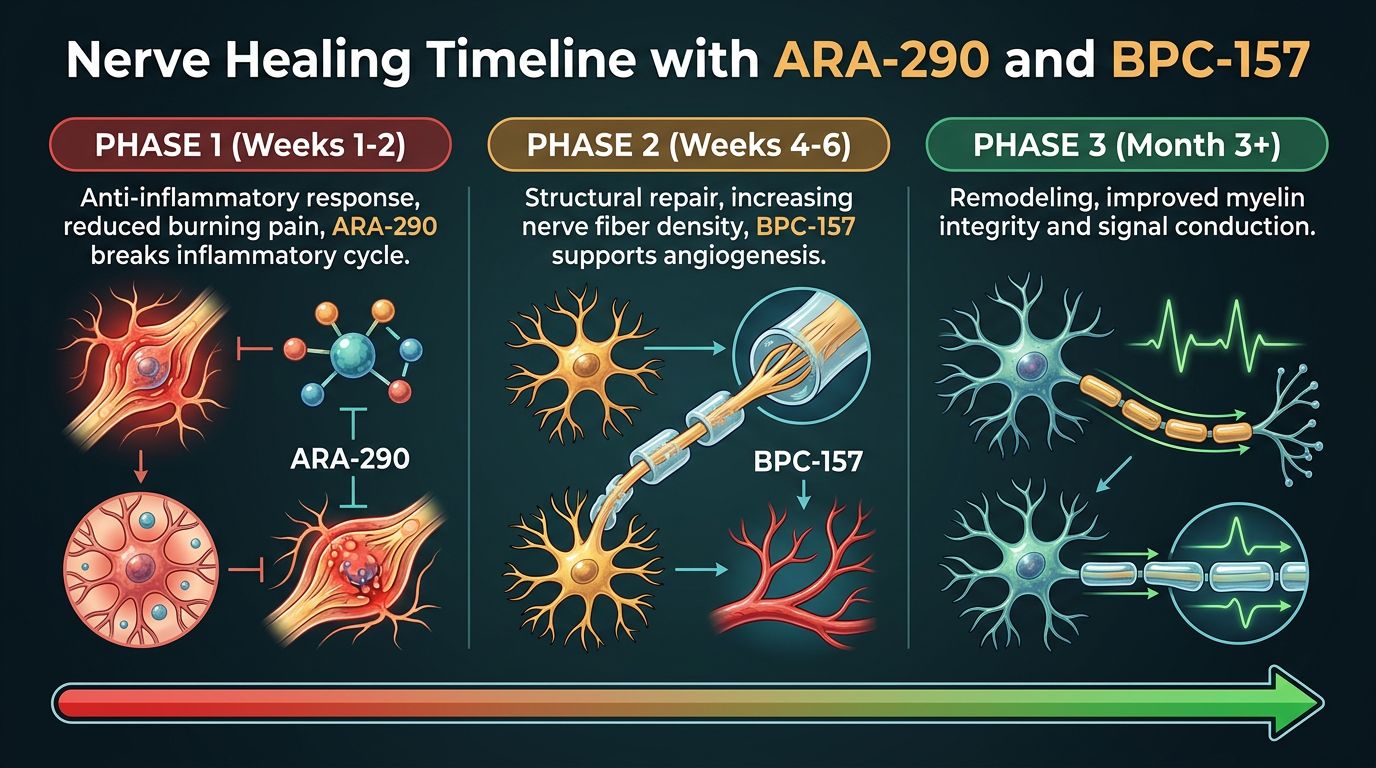
- Weeks 1-2: Anti-inflammatory effects are usually the first to be noticed. A reduction in the "burning" sensation is a common early marker in subject logs.
- Weeks 4-6: This is when structural changes often begin. In SFN studies, this is the window where nerve fiber density begins to statistically improve.
- Month 3+: Long-term remodeling. For severe neuropathy, research suggests sustained protocols are necessary to allow the nerve to regrow fully to its target.
Conclusion: The Future of Neuropathy
Peripheral nerve damage has long been a dark corner of medicine—a condition managed with painkillers but rarely cured. The emergence of ARA-290 and its partnership with BPC-157 offers a glimpse into a new era of proactive healing.
By moving beyond symptom management and targeting the root causes—blood flow, inflammation, and the Innate Repair Receptor—we are finally giving the body the tools it needs to rewire itself. Whether for recovering from an injury, managing autoimmune conditions, or simply optimizing long-term health, this synergistic stack represents the cutting edge of regenerative science.
As research continues, we expect to see these protocols refined and perhaps even integrated into standard care. For now, they remain powerful tools in the hands of educated researchers pushing the boundaries of what is possible in recovery.
Frequently Asked Questions
Can ARA-290 raise my red blood cell count like EPO?
No. ARA-290 is a "non-hematopoietic" analog of EPO. It has been chemically modified to remove the ability to stimulate bone marrow (which makes red blood cells) while retaining the ability to activate tissue repair. It targets the Innate Repair Receptor, not the EPO receptor responsible for carrying oxygen.
Is BPC-157 local or systemic?
BPC-157 is systemic, meaning it exerts effects throughout the body regardless of where it is administered. However, for specific injuries (like a damaged nerve in the leg), many researchers prefer administering it near the site to maximize local concentration, though the science supports its efficacy via systemic absorption as well.
Are there side effects to activating the Innate Repair Receptor?
Currently, the IRR seems to be a "safe switch." It is naturally designed to be turned on during injury. Studies on ARA-290 generally show a very high safety profile with few side effects, likely because it mimics a natural regulatory mechanism of the body.
Can I mix BPC-157 and ARA-290 in the same syringe?
In a research setting, this is often done to minimize the number of injections. Both are water-soluble peptides. However, standard laboratory practice usually suggests verifying the compatibility of specific distinct formulations before mixing.
References
- 1. Brines, M., & Cerami, A. (2005). The innate repair receptor: a multi-level defense system. Molecular Medicine, 11(1), 26–68.
- 2. Heung, M., & Brines, M. (2012). ARA290, a nonerythropoietic peptide engineered from erythropoietin, improves metabolic control and neuropathic pain in spontaneous type 2 diabetes. Molecular Medicine, 18(1), 123–138.
- 3. Sikiric, P., et al. (2010). Stable gastric pentadecapeptide BPC 157 in trials for inflammatory bowel disease (PL-10, PLD-116, PLD-148, PL-1415), wound healing, and vascular blockage. Current Pharmaceutical Design, 16(10), 1224–1234.
- 4. Culver, D. A., et al. (2013). Cibinetide (ARA 290) for the treatment of small fiber neuropathy in sarcoidosis. Expert Opinion on Investigational Drugs, 26(11), 1289–1296.
- 5. Gwathmey, T. M., et al. (2011). Nuclear factor-κB signaling in the pathogenesis of diabetic neuropathy. Antioxidants & Redox Signaling, 14(3), 469–480.
- 6. Sikiric, P., et al. (2016). Brain-gut axis and pentadecapeptide BPC 157: Theoretical and practical implications. Current Neuropharmacology, 14(8), 857–865.
- 7. Dahan, A., et al. (2013). ARA 290 improves symptoms in patients with sarcoidosis-associated small fiber neuropathy and impairs immune function. Molecular Medicine, 19(1), 334–345.
- 8. Seiwerth, S., et al. (2018). BPC 157 and standard angiogenic growth factors. Current Pharmaceutical Design, 24(18), 1972–1989.
- 9. Chen, H., et al. (2015). Erythropoietin signaling promotes regeneration of the transected sciatic nerve. Neural Regeneration Research, 10(4), 629–636.
- 10. Chang, C. H., et al. (2011). The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. Journal of Applied Physiology, 110(3), 774–780.
All research information is for educational purposes only. The statements made within this website have not been evaluated by the US Food and Drug Administration. The statements and the products of this company are not intended to diagnose, treat, cure or prevent any disease.